Department of Statistics, University of Warwick, Coventry, CV4 7AL, UK.
MRC Centre for Global Infectious Disease Analysis, Abdul Latif Jameel Institute for Disease and Emergency Analytics (J-IDEA), Imperial College London, London, UK.
BMC Med. 2021 Aug 30;19(1):213. doi: 10.1186/s12916-021-02096-0.
The literature paints a complex picture of the association between mortality risk and ICU strain. In this study, we sought to determine if there is an association between mortality risk in intensive care units (ICU) and occupancy of beds compatible with mechanical ventilation, as a proxy for strain.
A national retrospective observational cohort study of 89 English hospital trusts (i.e. groups of hospitals functioning as single operational units). Seven thousand one hundred thirty-three adults admitted to an ICU in England between 2 April and 1 December, 2020 (inclusive), with presumed or confirmed COVID-19, for whom data was submitted to the national surveillance programme and met study inclusion criteria. A Bayesian hierarchical approach was used to model the association between hospital trust level (mechanical ventilation compatible), bed occupancy, and in-hospital all-cause mortality. Results were adjusted for unit characteristics (pre-pandemic size), individual patient-level demographic characteristics (age, sex, ethnicity, deprivation index, time-to-ICU admission), and recorded chronic comorbidities (obesity, diabetes, respiratory disease, liver disease, heart disease, hypertension, immunosuppression, neurological disease, renal disease).
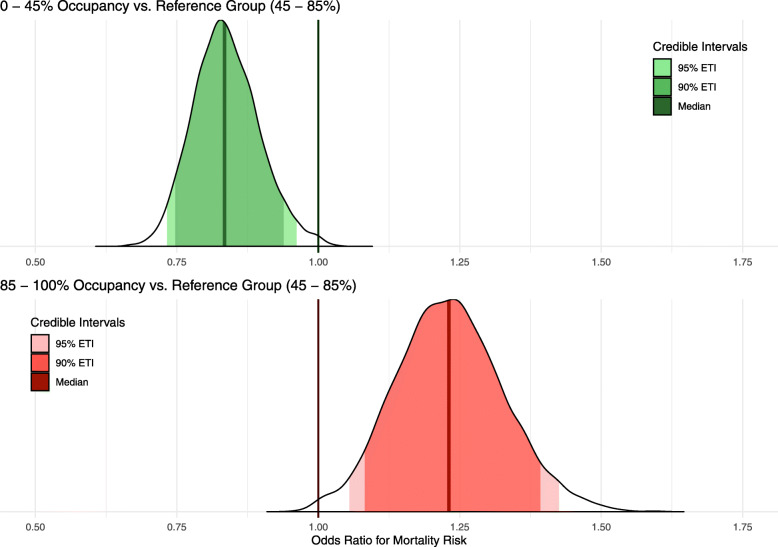
One hundred thirty-five thousand six hundred patient days were observed, with a mortality rate of 19.4 per 1000 patient days. Adjusting for patient-level factors, mortality was higher for admissions during periods of high occupancy (> 85% occupancy versus the baseline of 45 to 85%) [OR 1.23 (95% posterior credible interval (PCI): 1.08 to 1.39)]. In contrast, mortality was decreased for admissions during periods of low occupancy (< 45% relative to the baseline) [OR 0.83 (95% PCI 0.75 to 0.94)].
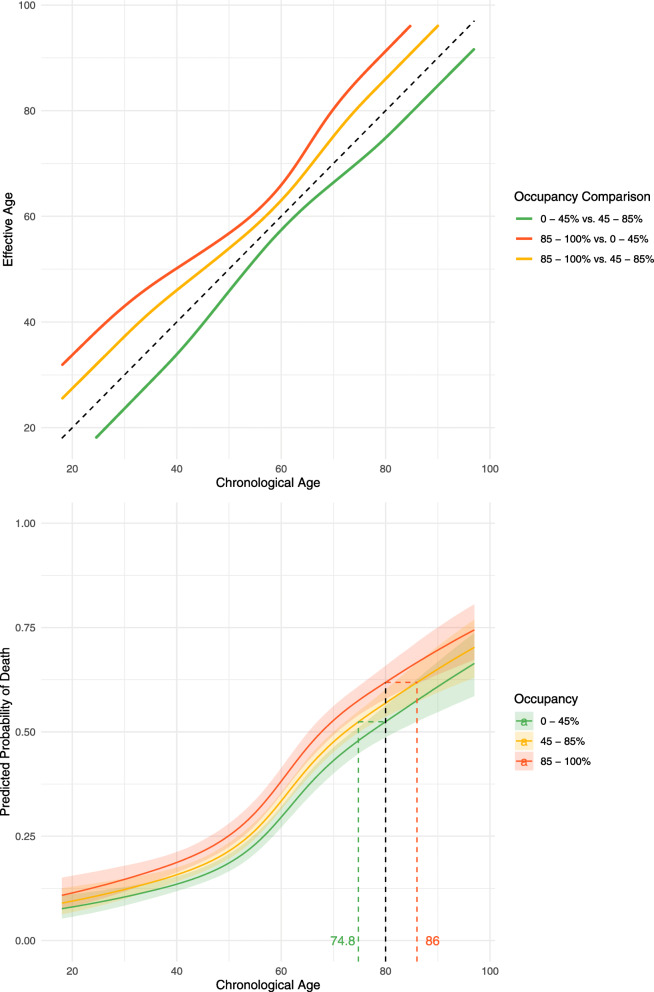
Increasing occupancy of beds compatible with mechanical ventilation, a proxy for operational strain, is associated with a higher mortality risk for individuals admitted to ICU. Further research is required to establish if this is a causal relationship or whether it reflects strain on other operational factors such as staff. If causal, the result highlights the importance of strategies to keep ICU occupancy low to mitigate the impact of this type of resource saturation.
文献描绘了死亡率风险与重症监护病房(ICU)紧张程度之间的复杂关系。在这项研究中,我们试图确定 ICU 死亡率与机械通气兼容床位的占用率之间是否存在关联,以作为紧张程度的替代指标。
这是一项全国性回顾性观察队列研究,共纳入了 89 家英国医院信托机构(即作为单一运营单位运作的一组医院)。2020 年 4 月 2 日至 12 月 1 日期间,英格兰 89 家 ICU 收治了 7133 名疑似或确诊 COVID-19 的成年人,且这些数据被提交至国家监测项目并符合研究纳入标准。采用贝叶斯分层方法来模拟医院信托级别(机械通气兼容)、床位占用率和院内全因死亡率之间的关系。结果调整了单位特征(大流行前规模)、个体患者层面的人口统计学特征(年龄、性别、种族、贫困指数、入住 ICU 时间)和记录的慢性合并症(肥胖、糖尿病、呼吸疾病、肝脏疾病、心脏病、高血压、免疫抑制、神经系统疾病、肾脏疾病)。
观察到 135600 个患者日,死亡率为每 1000 个患者日 19.4 例。在调整患者水平因素后,高床位占用率期间(>85%床位占用率,而基线为 45%至 85%)的死亡率更高[比值比(OR)1.23(95%置信区间(PCI):1.08 至 1.39)]。相比之下,低床位占用率期间(<45%,相对于基线)的死亡率降低[OR 0.83(95% PCI 0.75 至 0.94)]。
机械通气兼容床位占用率的增加,即操作紧张程度的替代指标,与 ICU 收治患者的死亡率风险增加相关。需要进一步研究以确定这是否是因果关系,还是反映了工作人员等其他操作因素的紧张程度。如果是因果关系,则该结果强调了保持 ICU 低床位占用率以减轻这种资源饱和类型的影响的策略的重要性。