Yuan Ye, Jian Jianing, Jing Hailiang, Yan Ran, You Fengming, Fu Xi, Du Linke, Li Wenyuan
Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, China.
Sichuan Evidence-Based Medicine Center of Traditional Chinese Medicine, Chengdu, China.
Front Surg. 2021 Aug 23;8:704986. doi: 10.3389/fsurg.2021.704986. eCollection 2021.
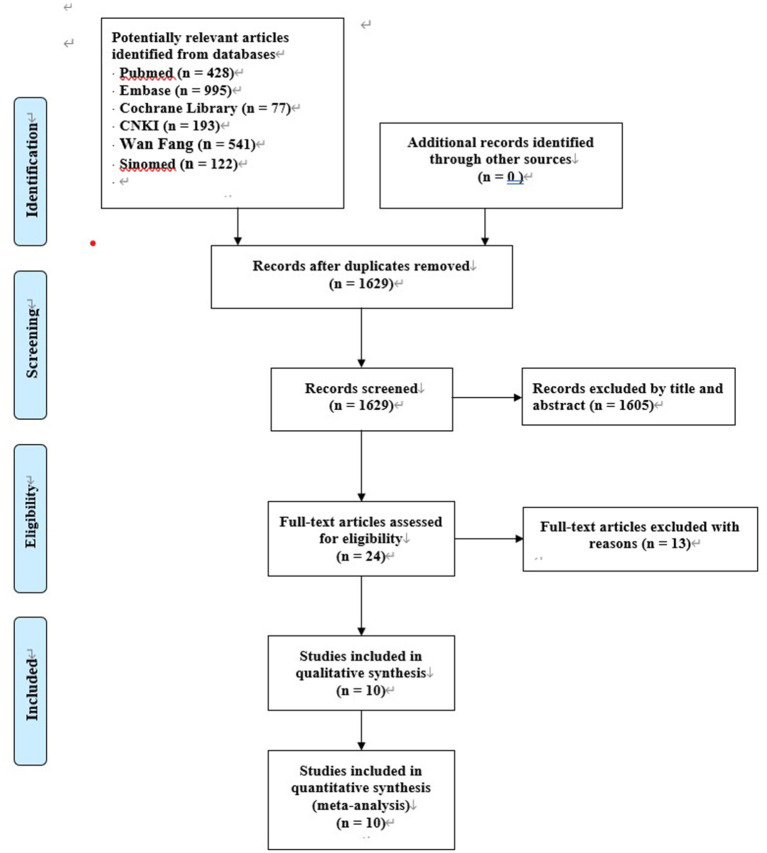
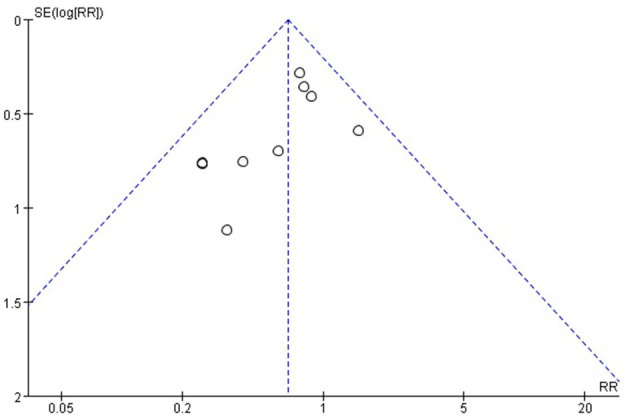
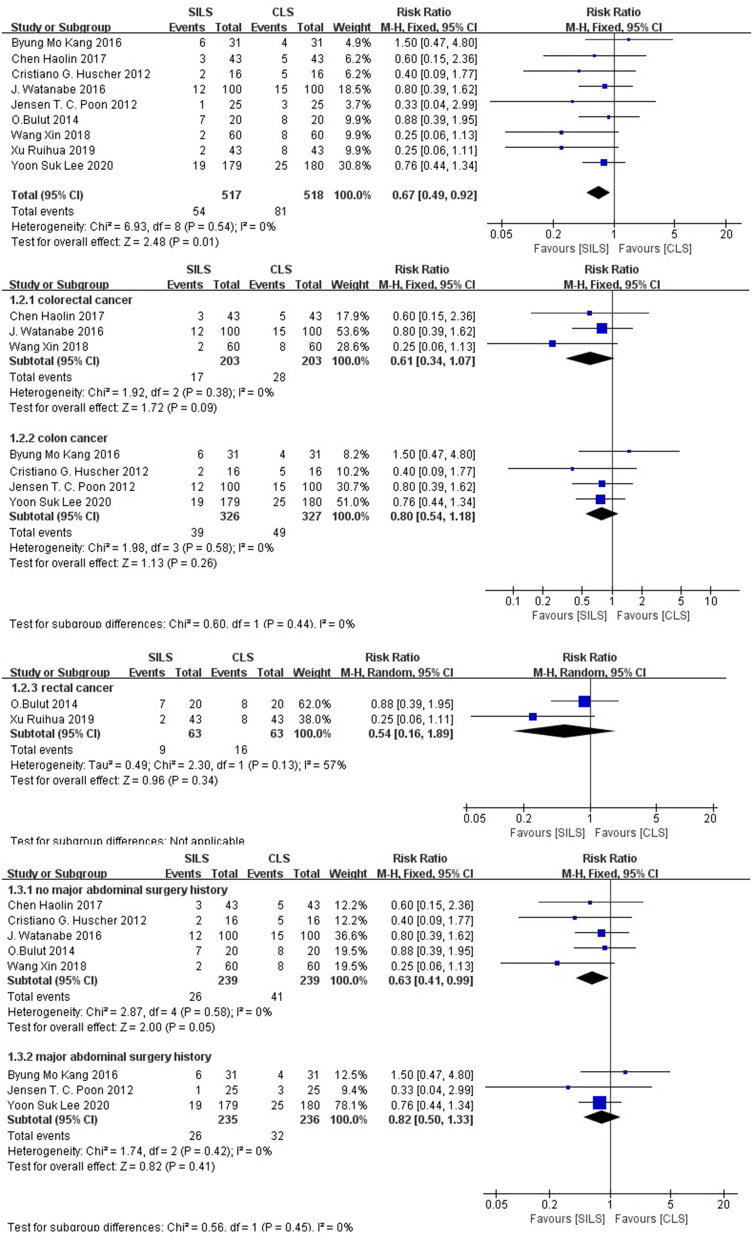
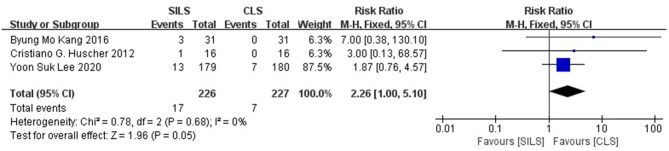
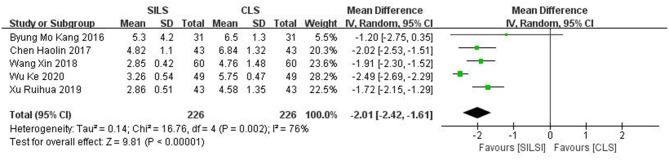
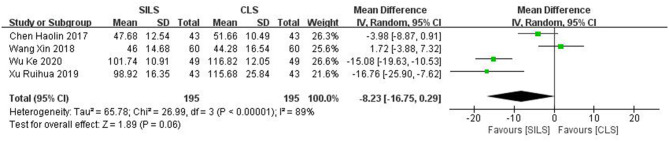
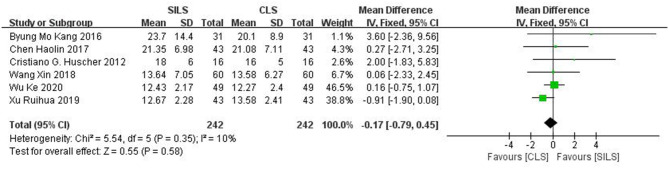
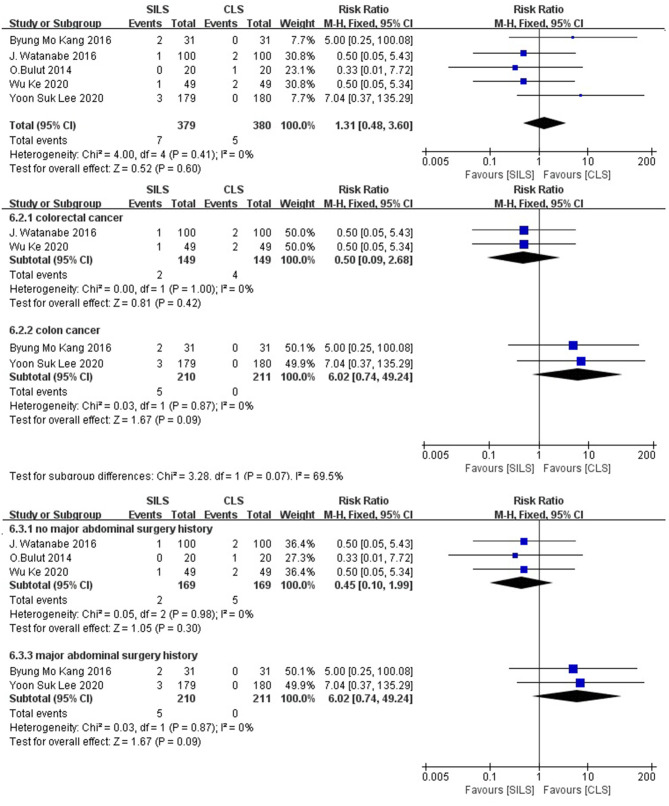
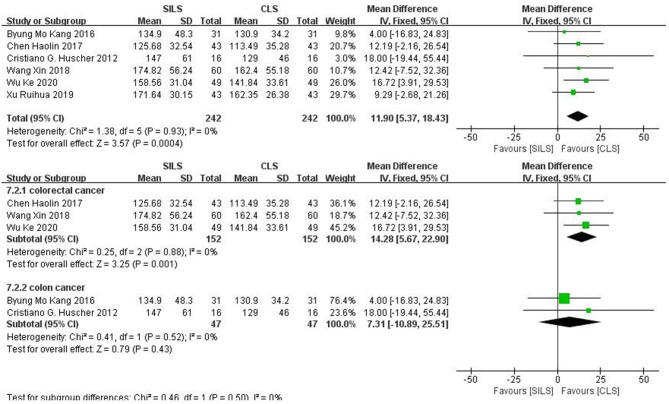
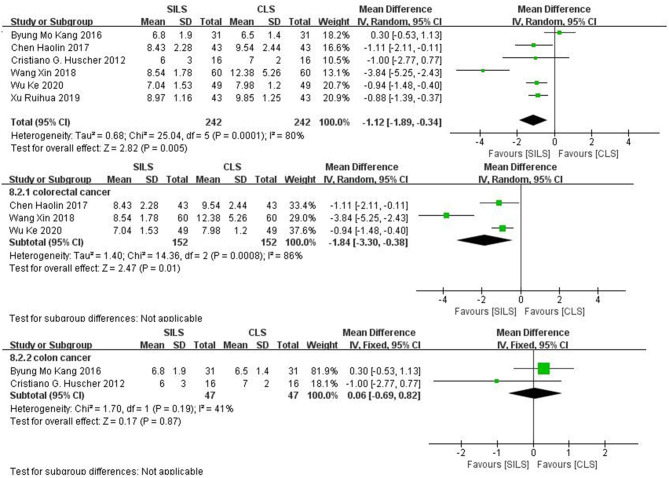
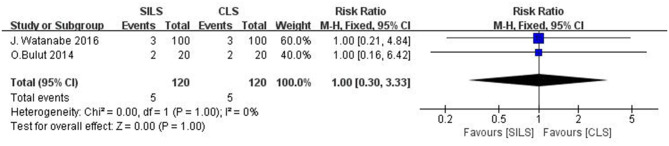
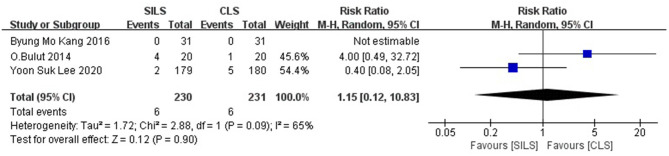
Although the advantages of single-incision laparoscopic surgery have been reported in several meta-analyses, the low quality of studies included in the meta-analyses limits the reliability of such a conclusion. In recent years, the number of randomized controlled trials on the efficacy of SILS in colorectal cancer has been on the rise. This update systematic review and meta-analysis of RCTs aims to compare efficacy and safety of SILS and CLS in the patients with colorectal cancer. Relevant data was searched on the CNKI, Wanfang, VIP, Sinomed, PubMed, Embase, and Cochrane CENTRAL databases from inception until February 5th, 2021. All RCTs comparing SILS and CLS were included. The main outcomes were 30 days of mortality, postoperative complications, intraoperative complications, whereas secondary outcomes were the number of lymph nodes removed, duration of hospital stay, intraoperative blood loss, abdominal incision length, reoperation, readmission, conversion to laparotomy, operation time and anastomotic leakage. A total of 10 RCTs were included, involving 1,133 participants. The quality of the included studies was generally high. No significant difference was found between SILS and CLS in the 30 days mortality rate. The results showed that SILS group had a lower rate of postoperative complications (RR = 0.67, 95% CI: 0.49-0.92), higher rate of intraoperative complications (RR = 2.26, 95%CI: 1.00-5.10), shorter length of abdominal incision (MD = -2.01, 95% CI:-2.42-1.61) (cm), longer operation time (MD = 11.90, 95% CI: 5.37-18.43) (minutes), shorter hospital stay (MD = -1.12, 95% CI: -1.89-0.34) (days) compared with CLS group. However, intraoperative blood loss (MD = -8.23, 95% CI: -16.75-0.29) (mL), number of lymph nodes removed (MD = -0.17, 95% CI: -0.79-0.45), conversion to laparotomy (RR=1.31, 95% CI: 0.48-3.60), reoperation (RR = 1.00, 95% CI: 0.30-3.33) and readmission (RR =1.15, 95% CI: 0.12-10.83) and anastomotic leakage were not significantly different between the two groups. These results indicate that SILS did not has a comprehensive and obvious advantage over the CLS. Surgeons and patients should carefully weigh the pros and cons of the two surgical procedures. Further RCTs are needed to prove long-term outcomes of SILS in colorectal cancer.
尽管多项荟萃分析报告了单孔腹腔镜手术的优势,但这些荟萃分析中纳入研究的质量较低,限制了这一结论的可靠性。近年来,关于单孔腹腔镜手术治疗结直肠癌疗效的随机对照试验数量不断增加。本次对随机对照试验的更新系统评价和荟萃分析旨在比较单孔腹腔镜手术(SILS)和传统腹腔镜手术(CLS)在结直肠癌患者中的疗效和安全性。从数据库建立至2021年2月5日,在知网、万方、维普、中国生物医学文献数据库、PubMed、Embase和Cochrane CENTRAL数据库中检索相关数据。纳入所有比较SILS和CLS的随机对照试验。主要结局指标为30天死亡率、术后并发症、术中并发症,次要结局指标为清扫淋巴结数量、住院时间、术中出血量、腹部切口长度、再次手术、再次入院、中转开腹、手术时间和吻合口漏。共纳入10项随机对照试验,涉及1133名参与者。纳入研究的质量总体较高。SILS和CLS在30天死亡率方面无显著差异。结果显示,与CLS组相比,SILS组术后并发症发生率较低(RR = 0.67,95%CI:0.49 - 0.92),术中并发症发生率较高(RR = 2.26,95%CI:1.00 - 5.10),腹部切口长度较短(MD = -2.01,95%CI:-2.42 - 1.61)(cm),手术时间较长(MD = 11.90,95%CI:5.37 - 18.43)(分钟),住院时间较短(MD = -1.12,95%CI:-1.89 - 0.34)(天)。然而,两组在术中出血量(MD = -8.23,95%CI:-16.75 - 0.29)(mL)、清扫淋巴结数量(MD = -0.17,95%CI:-0.79 - 0.45)、中转开腹(RR = 1.31,95%CI:0.48 - 3.60)、再次手术(RR = 1.00,95%CI:0.30 - 3.33)、再次入院(RR = 1.15,95%CI:0.12 - 10.83)和吻合口漏方面无显著差异。这些结果表明,SILS相对于CLS并没有全面且明显的优势。外科医生和患者应仔细权衡两种手术方式的利弊。需要进一步的随机对照试验来证实SILS治疗结直肠癌的长期疗效。