Division of Gastroenterology and Hepatology, University of Washington, Seattle, WA, USA.
Health Service Research and Development, Veterans Affairs Puget Sound Health Care System, Seattle, WA, USA.
Hepatol Commun. 2021 Dec;5(12):2080-2095. doi: 10.1002/hep4.1776. Epub 2021 Oct 3.
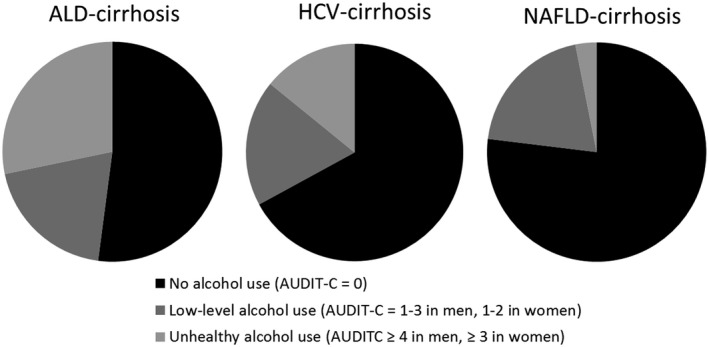
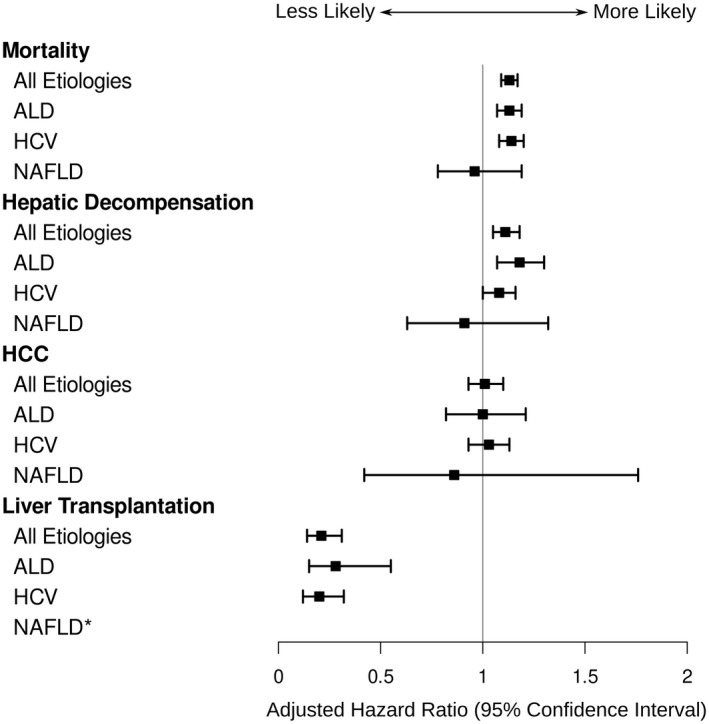
Alcohol use can cause hepatic necroinflammation and worsening portal hypertension in patients with cirrhosis. We aimed to evaluate the associations between degree of alcohol use and clinical liver-related outcomes according to etiology of cirrhosis. In this retrospective cohort analysis, 44,349 U.S. veterans with cirrhosis from alcohol-associated liver disease (ALD), chronic hepatitis C virus (HCV) infection, or nonalcoholic fatty liver disease were identified who completed the Alcohol Use Disorders Identification Test Consumption questionnaire in 2012. Based on this score, level of alcohol use was categorized as none, low level, or unhealthy. Multivariable Cox proportional hazards regression was used to assess for associations between alcohol use and mortality, cirrhosis decompensation (new ascites, encephalopathy, or variceal bleeding), and hepatocellular carcinoma (HCC). At baseline, 36.4% of patients endorsed alcohol use and 17.1% had unhealthy alcohol use. During a mean 4.9 years of follow-up, 25,806 (57.9%) patients died, 9,409 (21.4%) developed a new decompensation, and 4,733 (11.1%) developed HCC. In patients with ALD-cirrhosis and HCV-cirrhosis, unhealthy alcohol use, compared with no alcohol use, was associated with higher risks of mortality (adjusted hazard ratio [aHR] = 1.13, 95% confidence interval [CI] = 1.07-1.19 and aHR = 1.14, 95% CI = 1.08-1.20, respectively) and decompensation (aHR = 1.18, 95% CI = 1.07-1.30 and aHR = 1.08, 95% CI = 1.00-1.16, respectively). Alcohol use was not associated with HCC, regardless of cirrhosis etiology. Conclusion: Unhealthy alcohol use was common in patients with cirrhosis and was associated with higher risks of mortality and cirrhosis decompensation in patients with HCV-cirrhosis and ALD-cirrhosis. Therefore, health care providers should make every effort to help patients achieve abstinence. The lack of association between alcohol use and HCC merits further investigation.
酒精使用可导致肝硬化患者发生肝坏死性炎症和门静脉高压恶化。我们旨在根据肝硬化的病因评估酒精使用程度与临床肝脏相关结局之间的关联。在这项回顾性队列分析中,我们确定了 44349 名来自美国的患有酒精性肝病(ALD)、慢性丙型肝炎病毒(HCV)感染或非酒精性脂肪性肝病的肝硬化退伍军人,他们在 2012 年完成了酒精使用障碍识别测试消耗问卷。根据这个分数,酒精使用程度被分为无、低水平或不健康。多变量 Cox 比例风险回归用于评估酒精使用与死亡率、肝硬化失代偿(新发腹水、脑病或静脉曲张出血)和肝细胞癌(HCC)之间的关联。在基线时,36.4%的患者报告饮酒,17.1%的患者饮酒不健康。在平均 4.9 年的随访期间,25806(57.9%)名患者死亡,9409(21.4%)名患者发生新的失代偿,4733(11.1%)名患者发生 HCC。在 ALD 肝硬化和 HCV 肝硬化患者中,与不饮酒相比,不健康饮酒与更高的死亡率风险相关(调整后的危险比 [aHR] = 1.13,95%置信区间 [CI] = 1.07-1.19 和 aHR = 1.14,95%CI = 1.08-1.20)和失代偿(aHR = 1.18,95%CI = 1.07-1.30 和 aHR = 1.08,95%CI = 1.00-1.16)。无论肝硬化病因如何,酒精使用均与 HCC 无关。结论:肝硬化患者中常见不健康的饮酒行为,与 HCV 肝硬化和 ALD 肝硬化患者的死亡率和肝硬化失代偿风险增加相关。因此,医疗保健提供者应尽力帮助患者戒酒。酒精使用与 HCC 之间缺乏关联值得进一步研究。