Jacques Francois H, Nicholas Garth, Lorimer Ian A J, Sikati Foko Victorine, Prevost Jasmine, Dumais Nathalie, Milne Katy, Nelson Brad H, Woulfe John, Jansen Gerard, Apedaile B Erik
Clinique Neuro-Outaouais, Gatineau, Quebec, Canada.
Cancer Therapeutics Program, Ottawa Hospital Research Institute, Ottawa, Ontario, Canada.
Neurooncol Adv. 2021 Aug 25;3(1):vdab118. doi: 10.1093/noajnl/vdab118. eCollection 2021 Jan-Dec.
Glioblastoma (GBM) is known to use both local and systemic immunosuppressive strategies. One such strategy is the expression of the immune checkpoint protein programmed cell death ligand-1 (PD-L1) by both tumor cells and tumor-associated immune cells. Recent phase III trials using IgG4 antibodies targeting PD-1, the ligand for PD-L1, failed to show any benefit. Avelumab is an IgG1 monoclonal antibody targeting PD-L1. In contrast to the previously tested immune checkpoint inhibitors, it can directly bind tumor cells and immune cells expressing PD-L1 and can induce antibody-dependent cellular cytotoxicity.
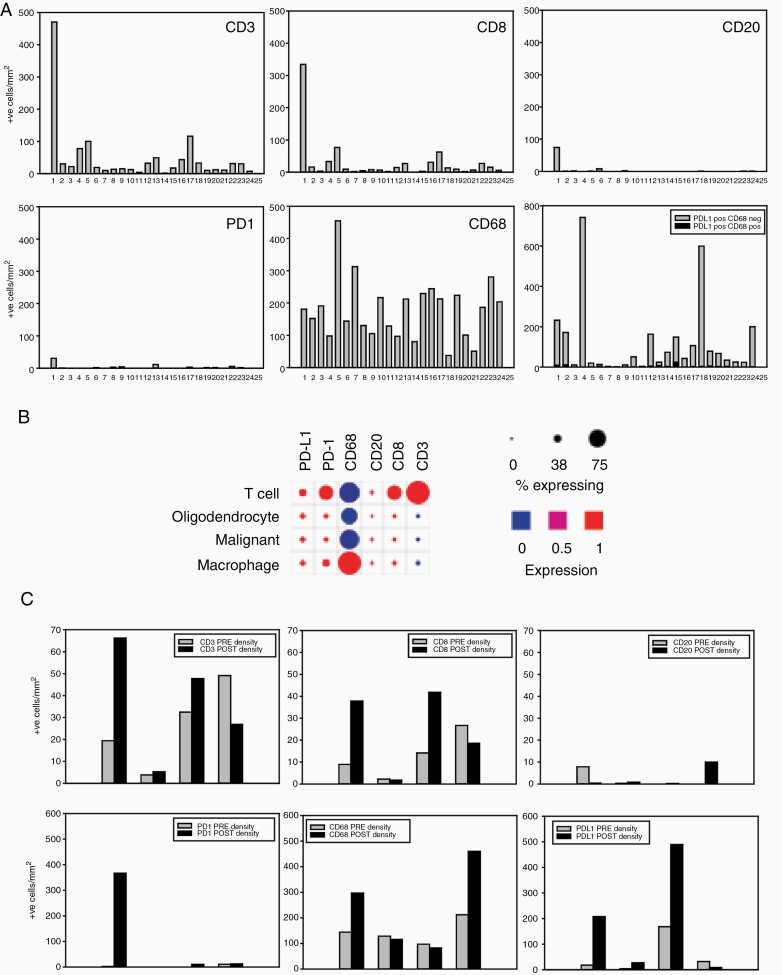
We conducted a single center, open label, phase II study where avelumab 10 mg/kg IV Q2W was added concurrently to the first monthly temozolomide cycle in patients with newly diagnosed GBM. Immunohistochemical analyses were performed on surgery samples. The primary objective was safety. Secondary objectives were efficacy outcomes according to the immunotherapy Response Assessment in Neuro Oncology criteria, progression free survival (PFS), and overall survival (OS). Exploratory objectives aimed at determining prognostic biomarkers.
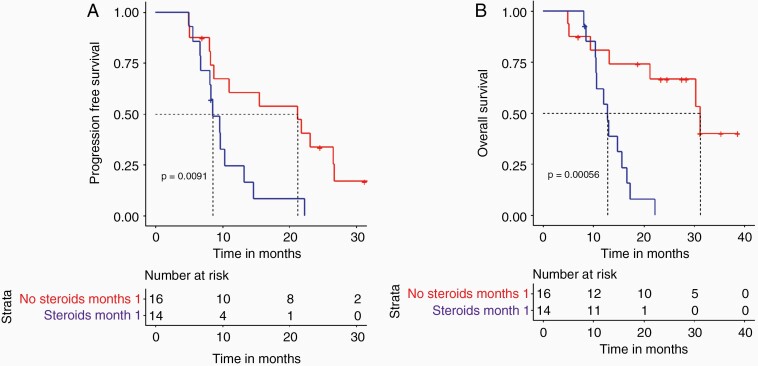
Thirty patients were started on therapy and two were lost to follow-up. Median follow-up time (reverse Kaplan-Meier) was 41.7 months (IQR: 28.3-43.4). Three (10.0%) patients had a related or possibly related treatment emergent adverse event that lead to transient or permanent discontinuation of avelumab. Eight (26.7%) patients had one or more immune-related adverse events, and 8 (26.7%) patients had an infusion-related reaction. The overall response rate was 23.3%, median PFS was 9.7 months, and the median OS was 15.3 months. No pretreatment biomarkers showed any predictive value.
The addition of avelumab to standard therapy in patients with GBM was not associated with any new safety signal. There was no apparent improvement in OS.
NCT03047473 Registered February 9, 2017.
已知胶质母细胞瘤(GBM)会采用局部和全身免疫抑制策略。其中一种策略是肿瘤细胞和肿瘤相关免疫细胞表达免疫检查点蛋白程序性细胞死亡配体1(PD-L1)。近期使用靶向PD-L1配体PD-1的IgG4抗体进行的III期试验未显示出任何益处。阿维鲁单抗是一种靶向PD-L1的IgG1单克隆抗体。与先前测试的免疫检查点抑制剂不同,它可以直接结合表达PD-L1的肿瘤细胞和免疫细胞,并可诱导抗体依赖性细胞毒性。
我们开展了一项单中心、开放标签的II期研究,在新诊断的GBM患者中,将阿维鲁单抗10mg/kg静脉注射,每2周一次,同时加入第一个月的替莫唑胺周期治疗。对手术样本进行免疫组织化学分析。主要目标是安全性。次要目标是根据神经肿瘤学免疫治疗反应评估标准得出的疗效结果、无进展生存期(PFS)和总生存期(OS)。探索性目标旨在确定预后生物标志物。
30例患者开始治疗,2例失访。中位随访时间(反向Kaplan-Meier法)为41.7个月(四分位间距:28.3 - 43.4)。3例(10.0%)患者发生了与治疗相关或可能相关的不良事件,导致阿维鲁单抗暂时或永久停用。8例(26.7%)患者发生了一种或多种免疫相关不良事件,8例(26.7%)患者发生了输液相关反应。总体缓解率为23.3%,中位PFS为9.7个月,中位OS为15.3个月。没有预处理生物标志物显示出任何预测价值。
在GBM患者的标准治疗中加入阿维鲁单抗未出现任何新的安全信号。OS没有明显改善。
NCT03047473,于2017年2月9日注册。