Department of Internal Medicine, Thun General Hospital, Thun, Switzerland.
Department of Emergency Medicine, Inselspital, University Hospital, University of Bern, Bern, Switzerland.
Crit Care. 2021 Oct 13;25(1):358. doi: 10.1186/s13054-021-03778-0.
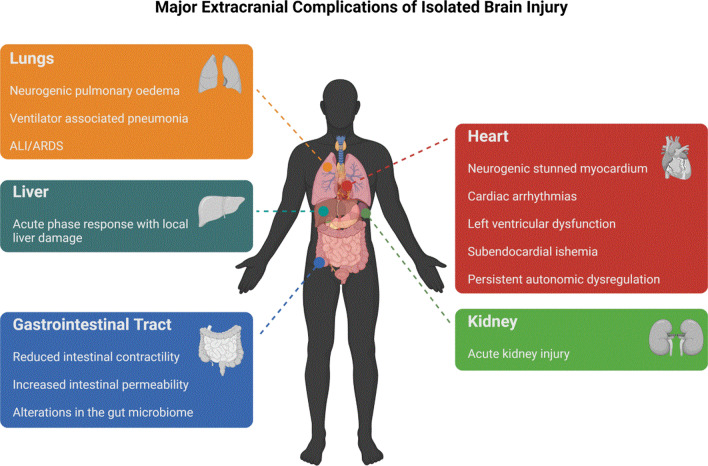
During the last decade, experimental and clinical studies have demonstrated that isolated acute brain injury (ABI) may cause severe dysfunction of peripheral extracranial organs and systems. Of all potential target organs and systems, the lung appears to be the most vulnerable to damage after brain injury (BI). The pathophysiology of these brain-lung interactions are complex and involve neurogenic pulmonary oedema, inflammation, neurodegeneration, neurotransmitters, immune suppression and dysfunction of the autonomic system. The systemic effects of inflammatory mediators in patients with BI create a systemic inflammatory environment that makes extracranial organs vulnerable to secondary procedures that enhance inflammation, such as mechanical ventilation (MV), surgery and infections. Indeed, previous studies have shown that in the presence of a systemic inflammatory environment, specific neurointensive care interventions-such as MV-may significantly contribute to the development of lung injury, regardless of the underlying mechanisms. Although current knowledge supports protective ventilation in patients with BI, it must be born in mind that ABI-related lung injury has distinct mechanisms that involve complex interactions between the brain and lungs. In this context, the role of extracerebral pathophysiology, especially in the lungs, has often been overlooked, as most physicians focus on intracranial injury and cerebral dysfunction. The present review aims to fill this gap by describing the pathophysiology of complications due to lung injuries in patients with a single ABI, and discusses the possible impact of MV in neurocritical care patients with normal lungs.
在过去的十年中,实验和临床研究已经证明,孤立性急性脑损伤(ABI)可能导致外周颅外器官和系统的严重功能障碍。在所有潜在的靶器官和系统中,肺似乎是脑损伤(BI)后最容易受损的器官。这些脑-肺相互作用的病理生理学非常复杂,涉及神经源性肺水肿、炎症、神经退行性变、神经递质、免疫抑制和自主神经系统功能障碍。BI 患者炎症介质的全身效应会产生全身性炎症环境,使颅外器官容易受到继发性增强炎症的程序的影响,如机械通气(MV)、手术和感染。事实上,先前的研究表明,在存在全身性炎症环境的情况下,特定的神经重症监护干预措施,如 MV,可能会显著促进肺损伤的发展,而与潜在机制无关。尽管目前的知识支持 BI 患者的保护性通气,但必须注意到,与 ABI 相关的肺损伤具有独特的机制,涉及大脑和肺部之间的复杂相互作用。在这种情况下,脑外病理生理学的作用,特别是在肺部,经常被忽视,因为大多数医生专注于颅内损伤和脑功能障碍。本综述旨在通过描述单一 ABI 患者肺损伤并发症的病理生理学来填补这一空白,并讨论 MV 在神经危重病患者正常肺中的可能影响。