Department of Infectious Disease, Faculty of Medicine, Imperial College London, London, UK.
Lung Division, Royal Brompton and Harefield Hospitals, Guy's and St. Thomas' NHS Foundation Trust, London, UK.
Nat Rev Immunol. 2021 Dec;21(12):762-768. doi: 10.1038/s41577-021-00631-x. Epub 2021 Oct 19.
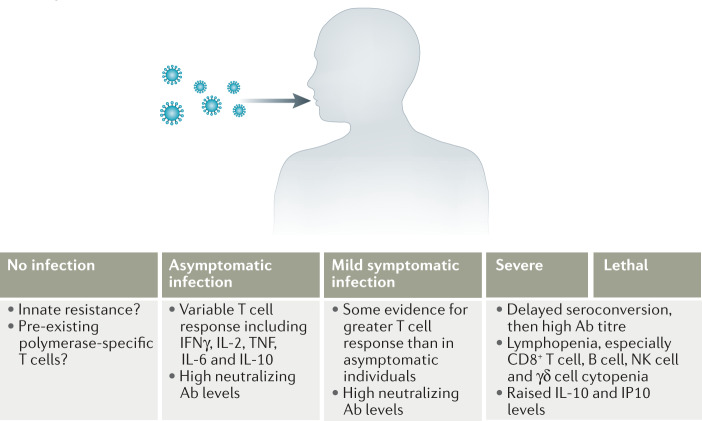
An important challenge during the COVID-19 pandemic has been to understand asymptomatic disease and the extent to which this may be a source of transmission. As asymptomatic disease is by definition hard to screen for, there is a lack of clarity about this aspect of the COVID-19 spectrum. Studies have considered whether the prevalence of asymptomatic disease is determined by differences in age, demographics, viral load, duration of shedding, and magnitude or durability of immunity. It is clear that adaptive immunity is strongly activated during asymptomatic infection, but some features of the T cell and antibody response may differ from those in symptomatic disease. Areas that need greater clarity include the extent to which asymptomatic disease leads to persistent symptoms (long COVID), and the quality, quantity and durability of immune priming required to confer subsequent protection.
在 COVID-19 大流行期间,一个重要的挑战是了解无症状疾病,以及它在多大程度上可能成为传播源。由于无症状疾病从定义上难以筛查,因此对于 COVID-19 谱的这一方面缺乏明确性。研究已经考虑了无症状疾病的患病率是否取决于年龄、人口统计学、病毒载量、脱落持续时间以及免疫的幅度或持久性等差异。很明显,适应性免疫在无症状感染期间被强烈激活,但 T 细胞和抗体反应的某些特征可能与有症状疾病不同。需要更明确的领域包括无症状疾病导致持续症状(长新冠)的程度,以及赋予后续保护所需的免疫启动的质量、数量和持久性。