Hurley Eoghan T, Hughes Andrew J, Jamal M Shazil, Mojica Edward S, Bloom David A, Youm Thomas, McCarthy Tom
New York University Langone Health, Department of Orthopaedic Surgery, New York, New York, U.S.A.
Sports Surgery Clinic, Dublin, Ireland.
Arthrosc Sports Med Rehabil. 2021 Aug 18;3(5):e1569-e1576. doi: 10.1016/j.asmr.2021.06.008. eCollection 2021 Oct.
The purpose of this study was to systematically review the evidence in the literature to ascertain whether acetabular labral repair (ALR) or debridement (ALD) resulted in superior patient outcomes.
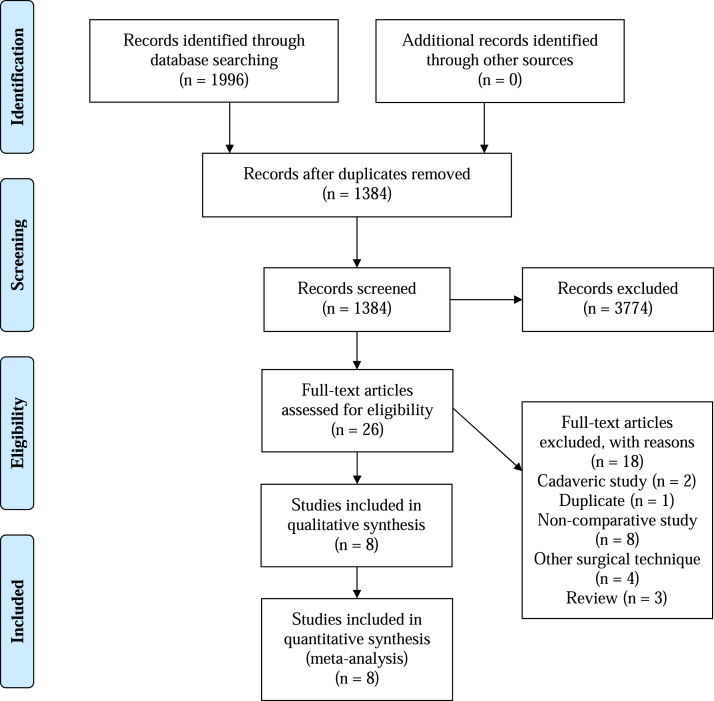
The systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Peer-reviewed studies comparing ALR and ALD published in English with full text available were included. Patients undergoing both open and arthroscopic surgery in randomized controlled trials, prospective cohort studies, retrospective cohort studies, and case-control studies were included. Studies were quantified for methodological quality using the MINORS criteria. Clinical outcomes were compared, with qualitative analysis, and quantitative analyses were performed using GraphPad Prism version 7. A value <.05 was considered to be statistically significant.
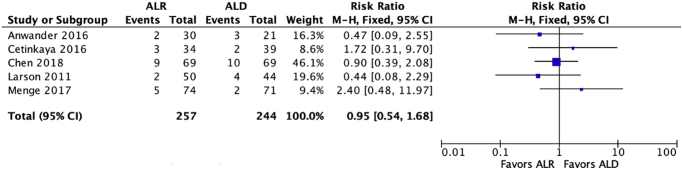
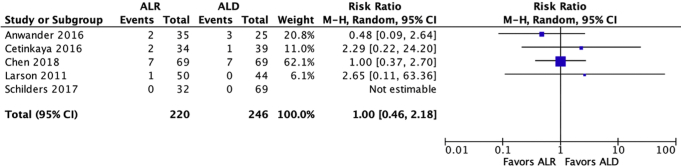
There were 8 studies included (level of evidence [LOE] I = 1; LOE II = 2; LOE III = 5). The 7 studies compared 364 patients (369 hips) with ALR to 318 patients (329 hips) with ALD, with a mean follow-up time ranging between 32-120 months. Five studies found significantly improved patient reported outcomes with ALR (Harris Hip Score, Merle d'Aubigné, Pain, SF-12). Several studies compared the outcomes after ALR and ALD and found statistical significance in all investigated metrics in favor of ALR. One study found a significant improvement in abduction but no other study found any difference in range of motion. No study found any difference in complication rate, revision rate or conversion to total hip arthroplasty. Although, 2 studies found ALR reduced the rate of osteoarthritic progression.
Current literature suggests that acetabular labral repair may result in superior patient reported outcomes. However, there appears to be no significant difference in the rate of progression to total hip arthroplasty at up to 10-year follow-up.
Level III, systematic review of Level I, II, and III studies.
本研究旨在系统回顾文献证据,以确定髋臼唇缘修复术(ALR)或清创术(ALD)是否能带来更优的患者预后。
本系统评价按照系统评价与Meta分析的首选报告项目指南进行。纳入以英文发表且全文可获取的比较ALR和ALD的同行评审研究。纳入随机对照试验、前瞻性队列研究、回顾性队列研究和病例对照研究中接受开放手术和关节镜手术的患者。使用MINORS标准对研究的方法学质量进行量化。对临床结局进行定性分析比较,并使用GraphPad Prism 7版本进行定量分析。P值<0.05被认为具有统计学意义。
共纳入8项研究(证据等级[LOE]I = 1;LOE II = 2;LOE III = 5)。7项研究将364例接受ALR的患者(369髋)与318例接受ALD的患者(329髋)进行比较,平均随访时间为32至120个月。5项研究发现接受ALR的患者报告结局有显著改善(Harris髋关节评分、Merle d'Aubigné评分、疼痛、SF-12)。多项研究比较了ALR和ALD后的结局,发现在所有调查指标上均具有统计学意义,支持ALR。一项研究发现外展有显著改善,但其他研究未发现活动范围有任何差异。没有研究发现并发症发生率、翻修率或转为全髋关节置换术有任何差异。不过,2项研究发现ALR降低了骨关节炎进展率。
当前文献表明,髋臼唇缘修复术可能会带来更优的患者报告结局。然而,在长达10年的随访中,进展为全髋关节置换术的发生率似乎没有显著差异。
III级,对I级、II级和III级研究的系统评价。