Miyagawa Fumi, Ogawa Kohei, Hashimoto Takashi, Asada Hideo
Department of Dermatology, Nara Medical University School of Medicine, Kashihara, Japan.
Department of Dermatology, Osaka City University Graduate School of Medicine, Osaka, Japan.
Case Rep Dermatol. 2021 Sep 20;13(3):464-469. doi: 10.1159/000519022. eCollection 2021 Sep-Dec.
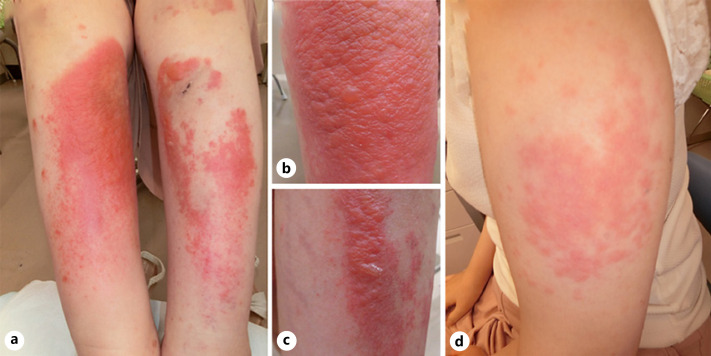
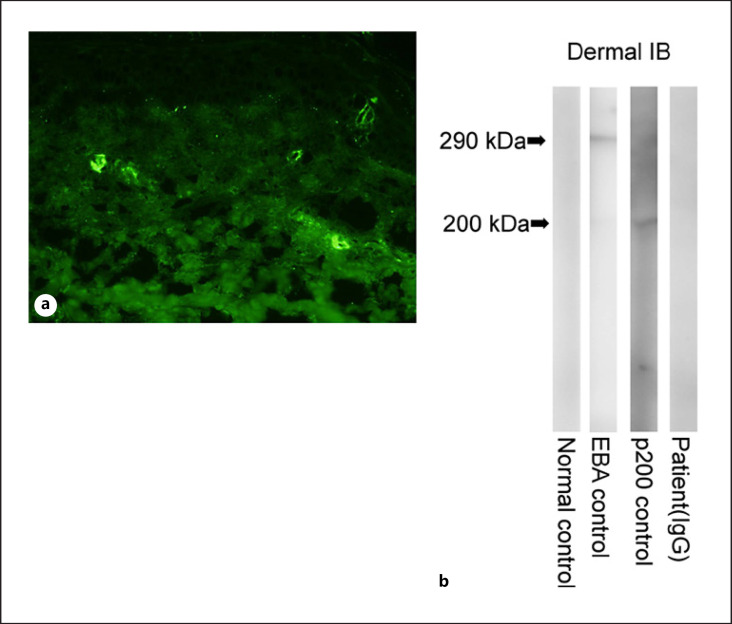
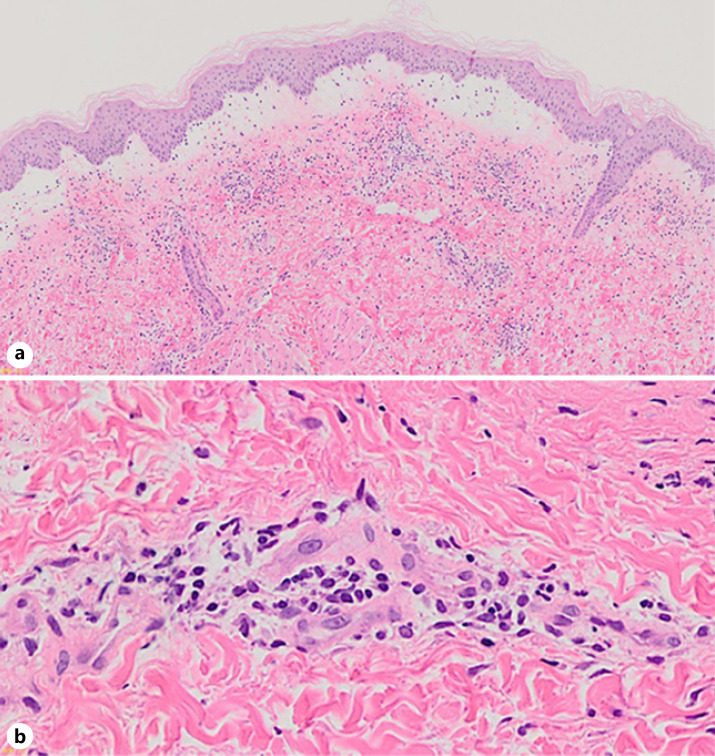
Rarely, patients with systemic lupus erythematosus (SLE) develop bullous eruptions, a disease called bullous SLE in a narrow sense that has autoantibodies against type VII collagen. We describe an unusual case in which a patient with SLE developed extensive bullae on her lower extremities. Histologically, the bullous lesions were suggestive of leukocytoclastic vasculitis with deposition of C3 within blood vessel walls. Immunoblot analyses and enzyme-linked immunosorbent assays were negative for anti-type VII collagen antibodies. We initially considered bullous SLE, but eventually made a diagnosis of secondary vasculitis in SLE. The oral prednisolone dose was increased, and the vesiculobullous lesions resolved. The clinical presentations of cutaneous vasculitis in SLE include palpable purpura, petechiae, papulonodular lesions, and livedo reticularis. Bullous lesions seem to be uncommon. Physicians need to be aware that extensive bullae can occur as a result of secondary vasculitis in SLE, even if the patient does not exhibit high disease activity.
系统性红斑狼疮(SLE)患者很少出现大疱性皮疹,狭义上这种疾病称为大疱性SLE,存在抗VII型胶原蛋白自身抗体。我们描述了1例不寻常病例,1名SLE患者双下肢出现广泛大疱。组织学上,大疱性病变提示白细胞破碎性血管炎,血管壁内有C3沉积。免疫印迹分析和酶联免疫吸附测定抗VII型胶原蛋白抗体均为阴性。我们最初考虑为大疱性SLE,但最终诊断为SLE继发性血管炎。口服泼尼松龙剂量增加,水疱大疱性病变消退。SLE皮肤血管炎的临床表现包括可触及的紫癜、瘀点、丘疹结节性病变和网状青斑。大疱性病变似乎并不常见。医生需要意识到,即使患者没有表现出高疾病活动度,SLE继发性血管炎也可能导致广泛大疱。