Guha Avirup, Wang Xiaoling, Harris Ryan A, Nelson Anna-Gay, Stepp David, Klaassen Zachary, Raval Priyanka, Cortes Jorge, Coughlin Steven S, Bogdanov Vladimir Y, Moore Justin X, Desai Nihar, Miller D Douglas, Lu Xin-Yun, Kim Ha Won, Weintraub Neal L
Harrington Heart and Vascular Institute, Case Western Reserve University, Cleveland, OH, United States.
Division of Cardiology, Department of Medicine, Medical College of Georgia at Augusta University, Augusta, GA, United States.
Front Cardiovasc Med. 2021 Oct 18;8:761488. doi: 10.3389/fcvm.2021.761488. eCollection 2021.
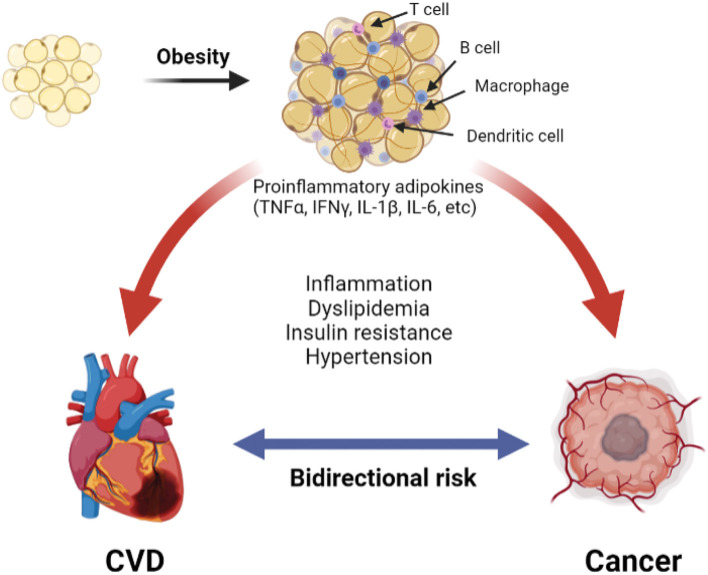
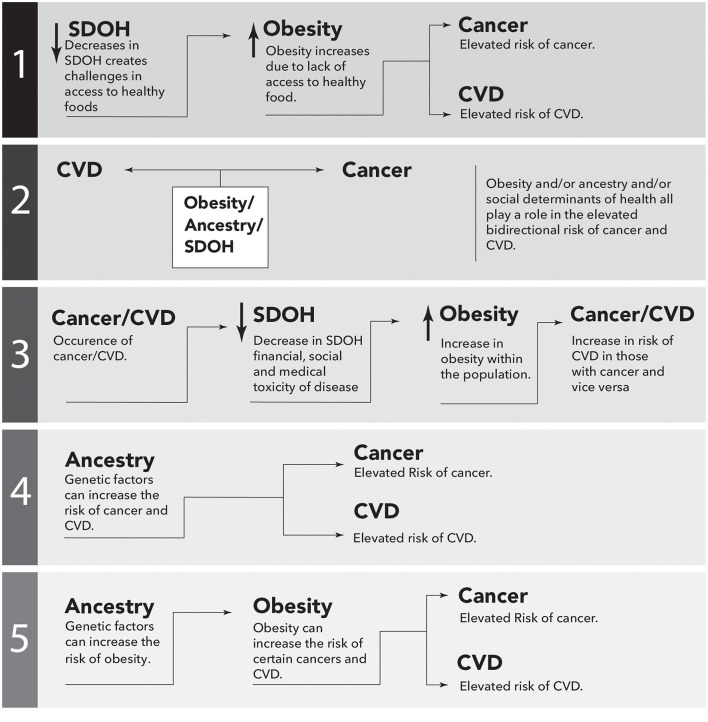
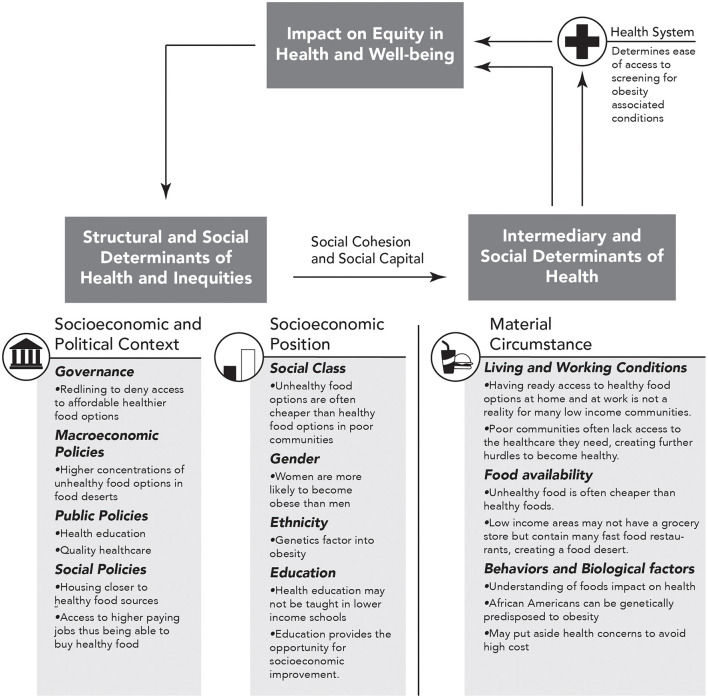
Cardiovascular disease (CVD) and cancer often occur in the same individuals, in part due to the shared risk factors such as obesity. Obesity promotes adipose inflammation, which is pathogenically linked to both cardiovascular disease and cancer. Compared with Caucasians, the prevalence of obesity is significantly higher in African Americans (AA), who exhibit more pronounced inflammation and, in turn, suffer from a higher burden of CVD and cancer-related mortality. The mechanisms that underlie this association among obesity, inflammation, and the bidirectional risk of CVD and cancer, particularly in AA, remain to be determined. Socio-economic disparities such as lack of access to healthy and affordable food may promote obesity and exacerbate hypertension and other CVD risk factors in AA. In turn, the resulting pro-inflammatory milieu contributes to the higher burden of CVD and cancer in AA. Additionally, biological factors that regulate systemic inflammation may be contributory. Mutations in atypical chemokine receptor 1 (ACKR1), otherwise known as the Duffy antigen receptor for chemokines (DARC), confer protection against malaria. Many AAs carry a mutation in the gene encoding this receptor, resulting in loss of its expression. ACKR1 functions as a decoy chemokine receptor, thus dampening chemokine receptor activation and inflammation. Published and preliminary data in humans and mice genetically deficient in ACKR1 suggest that this common gene mutation may contribute to ethnic susceptibility to obesity-related disease, CVD, and cancer. In this narrative review, we present the evidence regarding obesity-related disparities in the bidirectional risk of CVD and cancer and also discuss the potential association of gene polymorphisms in AAs with emphasis on ACKR1.
心血管疾病(CVD)和癌症常常在同一人群中发生,部分原因是存在肥胖等共同的风险因素。肥胖会引发脂肪组织炎症,而这种炎症在发病机制上与心血管疾病和癌症都有关联。与白种人相比,非裔美国人(AA)的肥胖患病率显著更高,他们表现出更明显的炎症,进而承受着更高的心血管疾病负担以及与癌症相关的死亡率。肥胖、炎症以及心血管疾病和癌症双向风险之间这种关联的潜在机制,尤其是在非裔美国人中,仍有待确定。诸如难以获得健康且价格合理的食物等社会经济差异,可能会促使非裔美国人肥胖,并加剧高血压及其他心血管疾病风险因素。反过来,由此产生的促炎环境又导致非裔美国人承受更高的心血管疾病和癌症负担。此外,调节全身炎症的生物学因素可能也有作用。非典型趋化因子受体1(ACKR1),即趋化因子达菲抗原受体(DARC)发生突变后可提供疟疾防护。许多非裔美国人在编码该受体的基因上携带一种突变,导致其表达缺失。ACKR1作为一种诱饵趋化因子受体,可抑制趋化因子受体激活和炎症反应。关于ACKR1基因缺陷的人类和小鼠的已发表及初步数据表明,这种常见基因突变可能导致种族对肥胖相关疾病、心血管疾病和癌症的易感性。在这篇叙述性综述中,我们展示了关于心血管疾病和癌症双向风险中与肥胖相关差异的证据,并讨论了非裔美国人基因多态性的潜在关联,重点是ACKR1。