Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy.
Department of Medicine, University of Perugia School of Medicine, Perugia, Italy; Center for Clinical and Translational Research-CERICLET, University of Perugia School of Medicine, Perugia, Italy.
Int J Cardiol. 2022 Jan 15;347:89-96. doi: 10.1016/j.ijcard.2021.10.156. Epub 2021 Nov 2.
Discrepant data were reported about hospital admissions for ST-segment elevation myocardial infarction (STEMI) during COVID-19 pandemic. We reviewed studies reporting STEMI hospitalizations during COVID-19 pandemic, investigating whether differences in COVID-19 epidemiology or public health-related factors could explain discrepant findings in different countries.
Search through MedLine, Embase, Scopus, Web-of-Science, Cochrane Register of Controlled Trials, of studies comparing STEMI admissions during COVID-19 pandemic with a reference period, without language restrictions, as registered in PROSPERO International Prospective Register of Systematic Reviews. Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines were followed. Data independently extracted by multiple investigators were pooled using a random-effects model. Health-related metrics were from publicly-available sources.
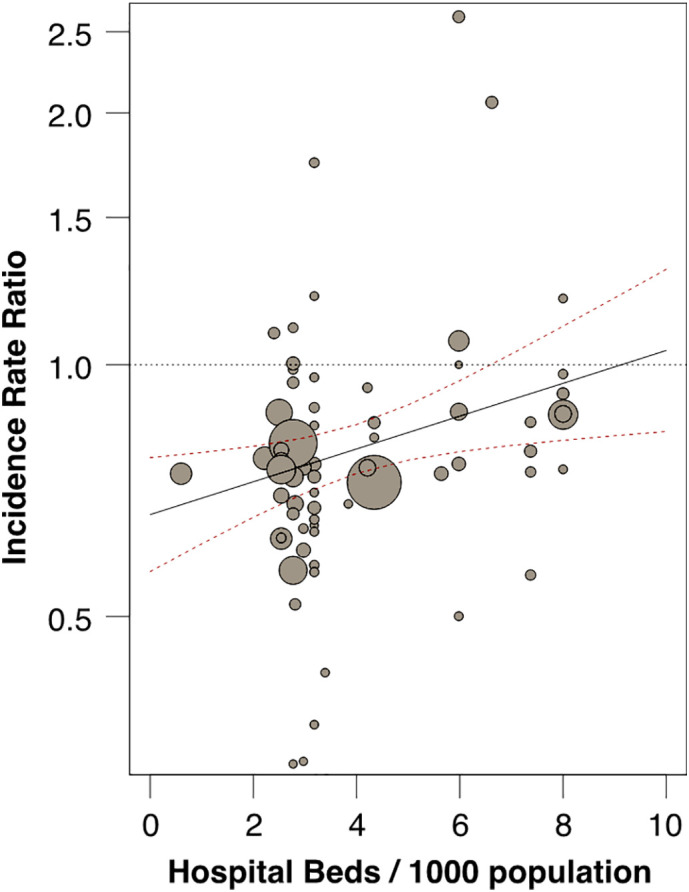
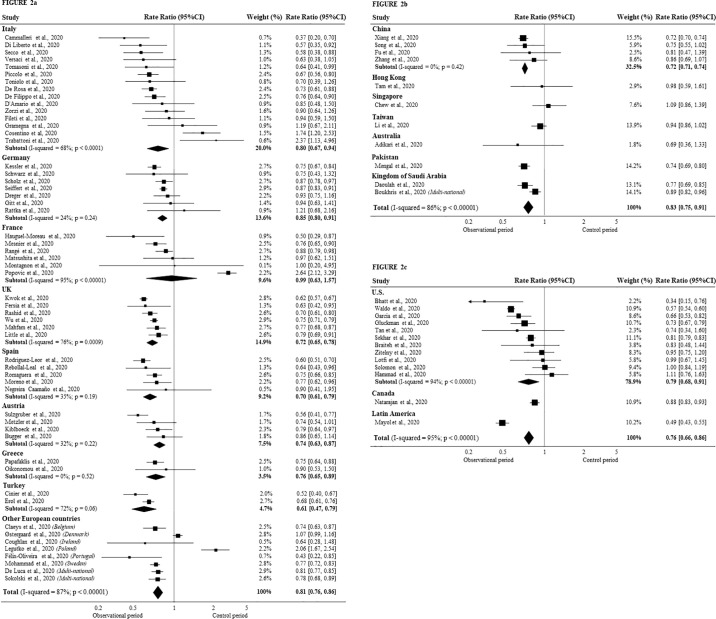
We included 79 articles (111,557 STEMI cases, from 57 countries). During peak COVID-19 pandemic, overall incidence rate-ratio (IRR) of STEMI hospitalizations over reference period decreased (0.80; 95% CI 0.76-0.84; p < 0.05). Although wide variations and significant heterogeneity were detected among studies (I = 89%; p < 0.0001), no significant differences were observed by report methodology (survey vs registry), or observation/reference period. However, large differences emerged at country level not explained by COVID-related epidemiological data, nor by public health strategies. Instead, IRRs for STEMI admissions were inversely related to hospital bed availability in each country (p < 0.05).
During COVID-19 pandemic hospitalization for STEMI significantly decreased, although to a smaller extent than initially reported. Large variability emerged across countries, unrelated to COVID-related epidemiology or social containment measures. Disparities in healthcare organization likely contributed, indicating that proper organization of emergency medicine should be preserved during pandemics.
关于 COVID-19 大流行期间 ST 段抬高型心肌梗死(STEMI)的住院数据存在差异。我们回顾了报告 COVID-19 大流行期间 STEMI 住院情况的研究,研究了 COVID-19 流行病学或与公共卫生相关的因素差异是否可以解释不同国家之间的不一致发现。
通过 MedLine、Embase、Scopus、Web-of-Science、Cochrane 对照试验登记册,对没有语言限制的 COVID-19 大流行期间与参考期比较 STEMI 入院的研究进行检索,这些研究均已在 PROSPERO 国际系统评价注册中心注册。研究遵循了系统评价和荟萃分析的 Preferred Reporting Items(PRISMA)指南。由多名研究人员独立提取的数据使用随机效应模型进行汇总。健康相关指标来自公开来源。
我们纳入了 79 篇文章(111,557 例 STEMI 病例,来自 57 个国家)。在 COVID-19 大流行高峰期,STEMI 住院的总发病率比值(IRR)与参考期相比下降(0.80;95%CI 0.76-0.84;p<0.05)。尽管研究之间存在广泛的差异和高度的异质性(I=89%;p<0.0001),但报告方法(调查与登记)或观察/参考期之间没有观察到显著差异。然而,在国家层面上存在很大差异,这些差异不能用 COVID 相关的流行病学数据或公共卫生策略来解释。相反,STEMI 入院的 IRR 与每个国家的病床可用性呈负相关(p<0.05)。
在 COVID-19 大流行期间,STEMI 的住院治疗显著减少,尽管减少的程度不如最初报告的那么大。各国之间出现了很大的差异,与 COVID 相关的流行病学或社会遏制措施无关。医疗保健组织的差异可能起了作用,这表明在大流行期间应保持急诊医学的适当组织。