Hu Qiang, Mao Weipu, Wu Tiange, Xu Zhipeng, Yu Junjie, Wang Can, Chen Saisai, Chen Shuqiu, Xu Bin, Xu Yueshuang, Chen Ming
Department of Urology, Zhongda Hospital, Southeast University, Nanjing, China.
Surgical Research Center, Institute of Urology, Southeast University Medical School, Nanjing, China.
Front Oncol. 2021 Oct 25;11:736640. doi: 10.3389/fonc.2021.736640. eCollection 2021.
This study aimed i) to identify the best cutoff points of neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) that predict sarcopenia and ii) to illustrate the association between sarcopenia risk and NLR or PLR in renal cell carcinoma (RCC) patients undergoing laparoscopic partial or radical nephrectomy.
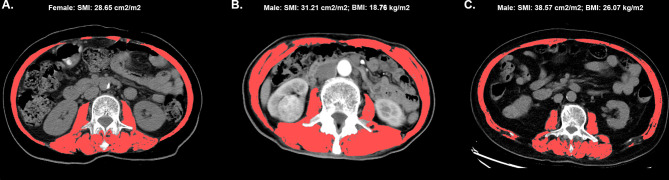
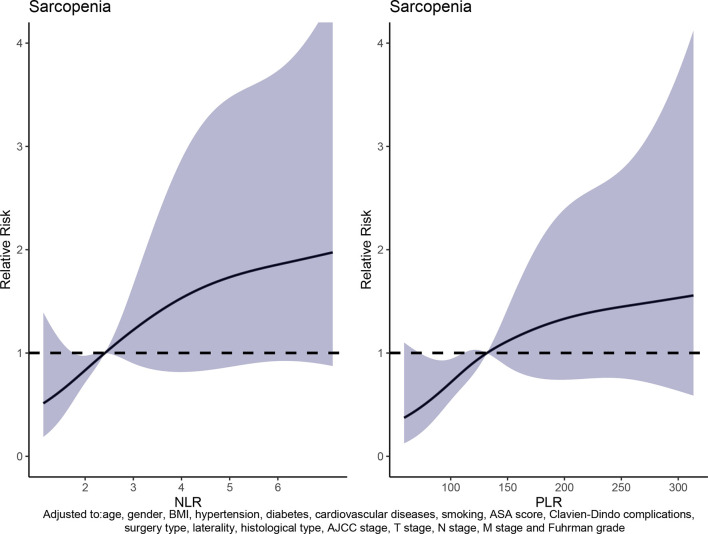
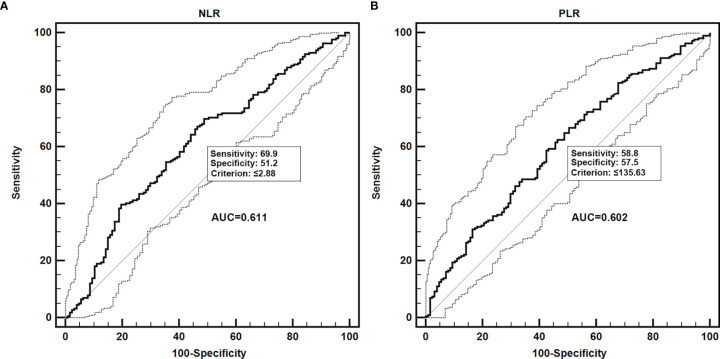
A total of 343 RCC patients who underwent laparoscopic partial or radical nephrectomy between 2014 and 2019 were enrolled in our study. Sarcopenia was assessed by lumbar skeletal muscle index (SMI). Receiver operating characteristic (ROC) curve was used to identify the best cutoff point of NLR or PLR to predict sarcopenia risk. Univariate and multivariate logistic regression and dose-response analysis curves of restricted cubic spline function were conducted to assess the relationship between sarcopenia and NLR or PLR.
The best cutoff points of NLR >2.88 or PLR >135.63 were confirmed by the ROC curve to predict sarcopenia risk. Dose-response curves showed that the risk of sarcopenia increased with raising NLR and PLR. Patients with NLR >2.88 or PLR >135.63 had a higher sarcopenia risk than those in the NLR ≤2.8 or PLR ≤135.63 group, respectively. By adjusting for all variables, we found that patients with NLR >2.88 and PLR >135.63 had 149% and 85% higher risk to develop sarcopenia, respectively, than those with NLR ≤2.8 (aOR = 2.49; 95% CI = 1.56-3.98; < 0.001) or PLR ≤135.63 (aOR = 1.85; 95% CI = 1.16-2.95; = 0.010).
In RCC patients receiving laparoscopic partial or radical nephrectomy, NLR and PLR, which were biomarkers of systemic inflammation, were associated with sarcopenia risk.
本研究旨在:i)确定预测肌肉减少症的中性粒细胞与淋巴细胞比值(NLR)和血小板与淋巴细胞比值(PLR)的最佳截断点;ii)阐明接受腹腔镜部分或根治性肾切除术的肾细胞癌(RCC)患者中肌肉减少症风险与NLR或PLR之间的关联。
本研究纳入了2014年至2019年间接受腹腔镜部分或根治性肾切除术的343例RCC患者。通过腰椎骨骼肌指数(SMI)评估肌肉减少症。采用受试者工作特征(ROC)曲线确定NLR或PLR预测肌肉减少症风险的最佳截断点。进行单因素和多因素逻辑回归以及限制立方样条函数的剂量反应分析曲线,以评估肌肉减少症与NLR或PLR之间的关系。
ROC曲线证实NLR>2.88或PLR>135.63的最佳截断点可预测肌肉减少症风险。剂量反应曲线显示,肌肉减少症风险随NLR和PLR升高而增加。NLR>2.88或PLR>135.63的患者肌肉减少症风险分别高于NLR≤2.8或PLR≤135.63组的患者。通过对所有变量进行调整,我们发现NLR>2.88和PLR>135.63的患者发生肌肉减少症的风险分别比NLR≤2.8(调整后比值比[aOR]=2.49;95%置信区间[CI]=1.56-3.98;P<0.001)或PLR≤135.63(aOR=1.85;95%CI=1.16-2.95;P=0.010)的患者高149%和85%。
在接受腹腔镜部分或根治性肾切除术的RCC患者中,作为全身炎症生物标志物的NLR和PLR与肌肉减少症风险相关。