Service de Médecine Intensive Réanimation, Hôpitaux Universitaires Henri Mondor, AP-HP, 1 rue Gustave Eiffel, 94010, Créteil Cedex, France.
CARMAS, Univ Paris Est Créteil, 94010, Créteil, France.
Crit Care. 2021 Nov 15;25(1):391. doi: 10.1186/s13054-021-03802-3.
Extubation failure is an important issue in ventilated patients and its risk factors remain a matter of research. We conducted a systematic review and meta-analysis to explore factors associated with extubation failure in ventilated patients who passed a spontaneous breathing trial and underwent planned extubation. This systematic review was registered in PROPERO with the Registration ID CRD42019137003.
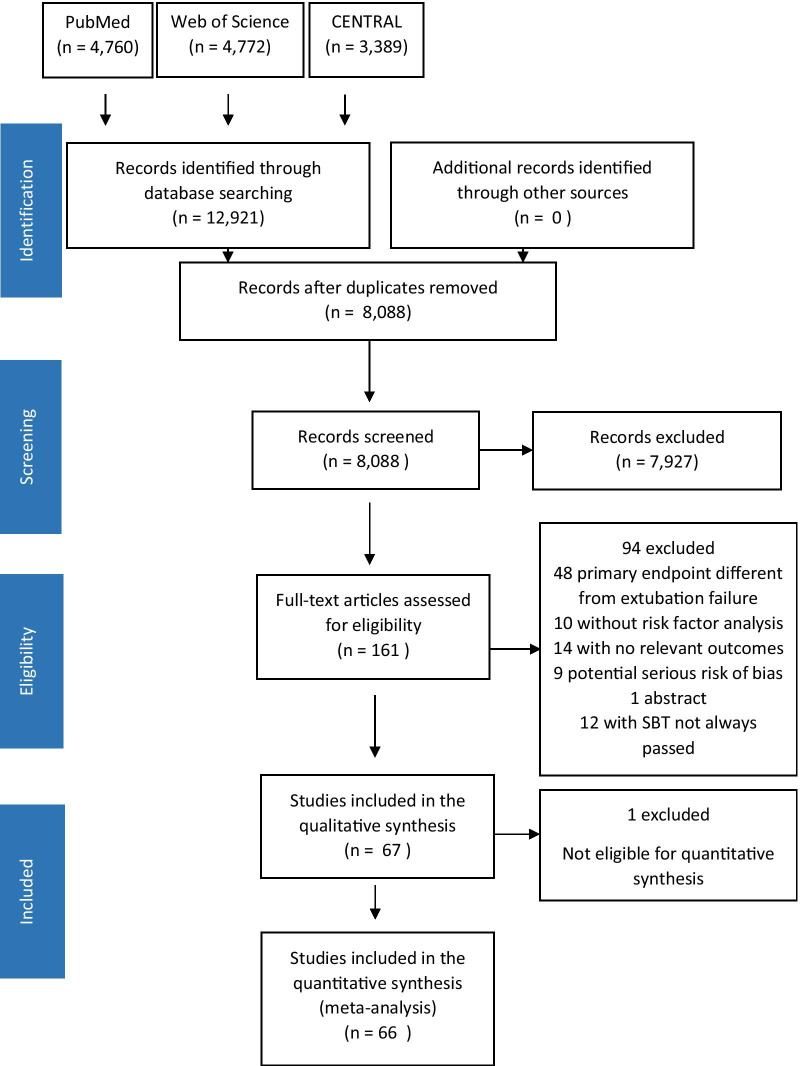
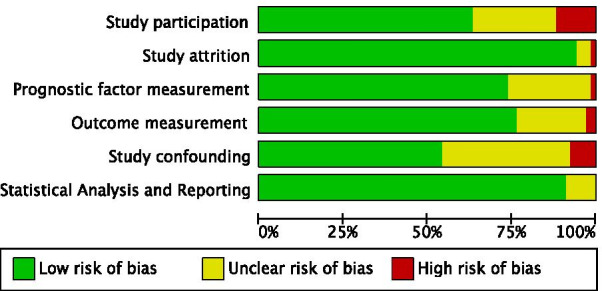
We searched the PubMed, Web of Science and Cochrane Controlled Register of Trials for studies published from January 1998 to December 2018. We included observational studies involving risk factors associated with extubation failure in adult intensive care unit patients who underwent invasive mechanical ventilation. Two authors independently extracted data and assessed the validity of included studies.
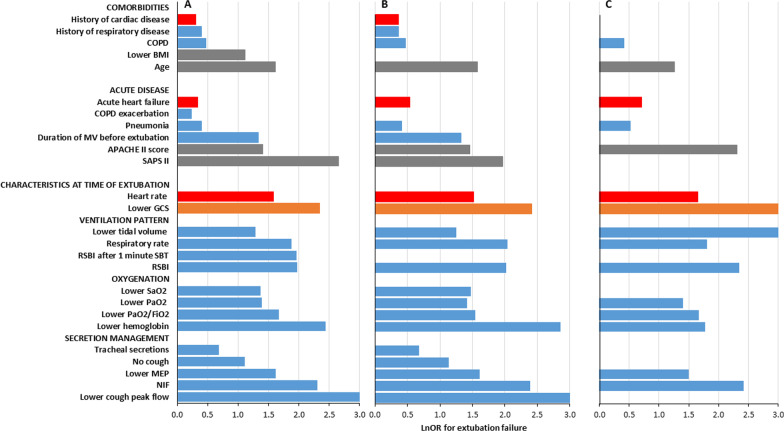
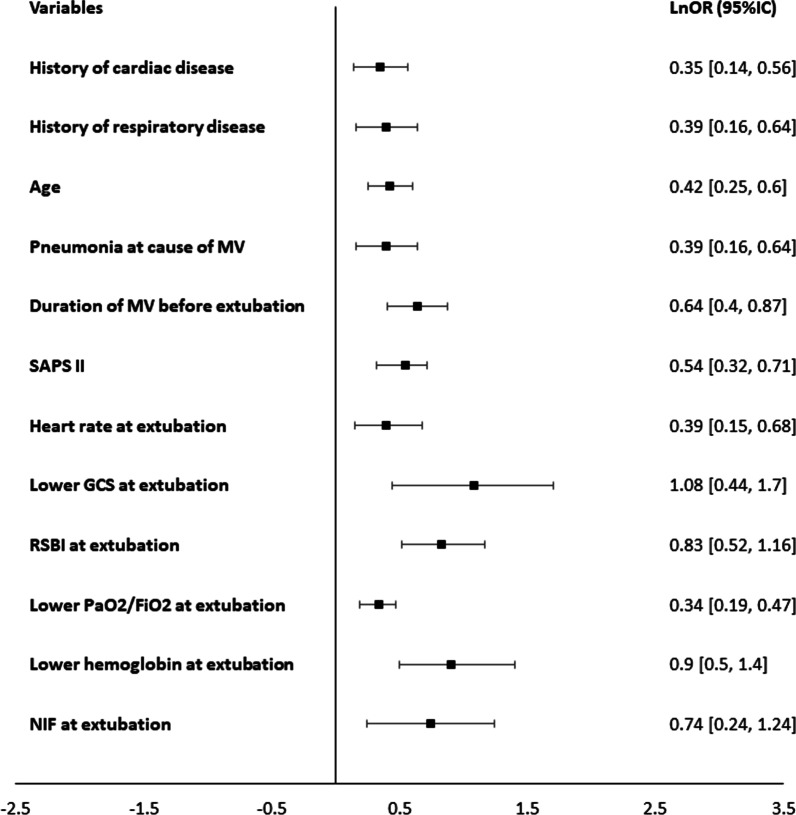
Sixty-seven studies (involving 26,847 participants) met the inclusion criteria and were included in our meta-analysis. We analyzed 49 variables and, among them, we identified 26 factors significantly associated with extubation failure. Risk factors were distributed into three domains (comorbidities, acute disease severity and characteristics at time of extubation) involving mainly three functions (circulatory, respiratory and neurological). Among these, the physiological respiratory characteristics at time of extubation were the most represented. The individual topic of secretion management was the one with the largest number of variables. By Bayesian multivariable meta-analysis, twelve factors were significantly associated with extubation failure: age, history of cardiac disease, history of respiratory disease, Simplified Acute Physiologic Score II score, pneumonia, duration of mechanical ventilation, heart rate, Rapid Shallow Breathing Index, negative inspiratory force, lower PaO/FiO ratio, lower hemoglobin level and lower Glasgow Coma Scale before extubation, with the latest factor having the strongest association with extubation outcome.
Numerous factors are associated with extubation failure in critically ill patients who have passed a spontaneous breathing trial. Robust multiparametric clinical scores and/or artificial intelligence algorithms should be tested based on the selected independent variables in order to improve the prediction of extubation outcome in the clinical scenario.
拔管失败是通气患者的一个重要问题,其危险因素仍然是研究的一个问题。我们进行了系统评价和荟萃分析,以探讨通过自主呼吸试验并计划进行拔管的通气患者中与拔管失败相关的因素。这项系统评价已在 PROPERO 中注册,注册号为 CRD42019137003。
我们检索了 1998 年 1 月至 2018 年 12 月期间发表的 PubMed、Web of Science 和 Cochrane 对照试验注册库中的研究。我们纳入了涉及接受有创机械通气的成人重症监护病房患者与拔管失败相关的危险因素的观察性研究。两位作者独立提取数据并评估纳入研究的有效性。
67 项研究(涉及 26847 名参与者)符合纳入标准并纳入荟萃分析。我们分析了 49 个变量,其中有 26 个因素与拔管失败显著相关。危险因素分布在三个领域(合并症、急性疾病严重程度和拔管时的特征),主要涉及三个功能(循环、呼吸和神经)。在这些因素中,拔管时的生理呼吸特征最为突出。分泌管理是变量最多的个别主题。通过贝叶斯多变量荟萃分析,有 12 个因素与拔管失败显著相关:年龄、心脏病史、呼吸系统疾病史、简化急性生理学评分 II 评分、肺炎、机械通气时间、心率、快速浅呼吸指数、负吸气力、较低的 PaO/FiO 比值、较低的血红蛋白水平和拔管前较低的格拉斯哥昏迷评分,其中最新的因素与拔管结果的相关性最强。
许多因素与通过自主呼吸试验的危重症患者的拔管失败相关。应该基于选定的独立变量测试稳健的多参数临床评分和/或人工智能算法,以提高临床情况下拔管结果的预测。