Radboud Institute for Health Sciences, Department of Physiology, Radboud University Medical Center, Nijmegen, the Netherlands.
Research Institute for Sports and Exercise Sciences, Liverpool John Moores University, Liverpool, United Kingdom.
PLoS Med. 2021 Dec 2;18(12):e1003845. doi: 10.1371/journal.pmed.1003845. eCollection 2021 Dec.
Moderate to vigorous physical activity (MVPA) is strongly associated with risk reductions of noncommunicable diseases and mortality. Cardiovascular health status may influence the benefits of MVPA. We compare the association between MVPA and incident major adverse cardiovascular events (MACE) and mortality between healthy individuals, individuals with elevated levels of cardiovascular risk factors (CVRF), and cardiovascular disease (CVD).
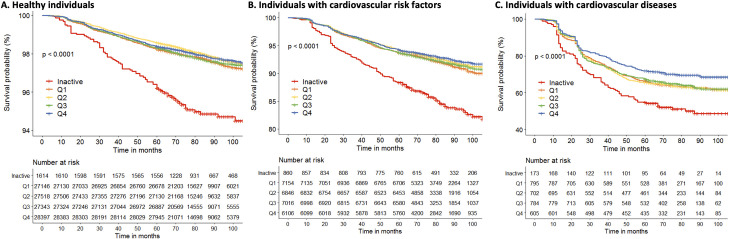
A cohort study was performed in the 3 northern provinces of the Netherlands, in which data were collected between 2006 and 2018, with a median follow-up of 6.8 years (Q25 5.7; Q75 7.9). A total of 142,493 participants of the Lifelines Cohort Study were stratified at baseline as (1) healthy; (2) CVRF; or (3) CVD. Individuals were categorized into "inactive" and 4 quartiles of least (Q1) to most (Q4) active based on self-reported MVPA volumes. Primary outcome was a composite of incident MACE and all-cause mortality during follow-up. Cox regression was used to estimate hazard ratios (HRs), 95% confidence intervals (CIs) and P values. The main analyses were stratified on baseline health status and adjusted for age, sex, income, education, alcohol consumption, smoking, protein, fat and carbohydrate intake, kidney function, arrhythmias, hypothyroid, lung disease, osteoarthritis, and rheumatoid arthritis. The event rates were 2.2% in healthy individuals (n = 2,485 of n = 112,018), 7.9% in those with CVRF (n = 2,214 of n = 27,982) and 40.9% in those with CVD (n = 1,019 of n = 2,493). No linear association between MVPA and all-cause mortality or MACE was found for healthy individuals (P = 0.36) and individuals with CVRF (P = 0.86), but a linear association was demonstrated for individuals with CVD (P = 0.04). Adjusted HRs in healthy individuals were 0.81 (95% CI 0.64 to 1.02, P = 0.07), 0.71 (95% CI 0.56 to 0.89, P = 0.004), 0.72 (95% CI 0.57 to 0.91, P = 0.006), and 0.76 (95% CI 0.60 to 0.96, P = 0.02) for MVPA Q1 to Q4, respectively, compared to inactive individuals. In individuals with CVRF, HRs were 0.69 (95% CI 0.57 to 0.82, P < 0.001), 0.66 (95% CI 0.55 to 0.80, P < 0.001), 0.64 (95% CI 0.53 to 0.77, P < 0.001), and 0.69 (95% CI 0.57 to 0.84, P < 0.001) for MVPA Q1 to Q4, respectively, compared to inactive individuals. Finally, HRs for MVPA Q1 to Q4 compared to inactive individuals were 0.80 (95% CI 0.62 to 1.03, P = 0.09), 0.82 (95% CI 0.63 to 1.06, P = 0.13), 0.74 (95% CI 0.57 to 0.95, P = 0.02), and 0.70 (95% CI 0.53 to 0.93, P = 0.01) in CVD patients. Leisure MVPA was associated with the most health benefits, nonleisure MVPA with little health benefits, and occupational MVPA with no health benefits. Study limitations include its observational nature, self-report data about MVPA, and potentially residual confounding despite extensive adjustment for lifestyle risk factors and health-related factors.
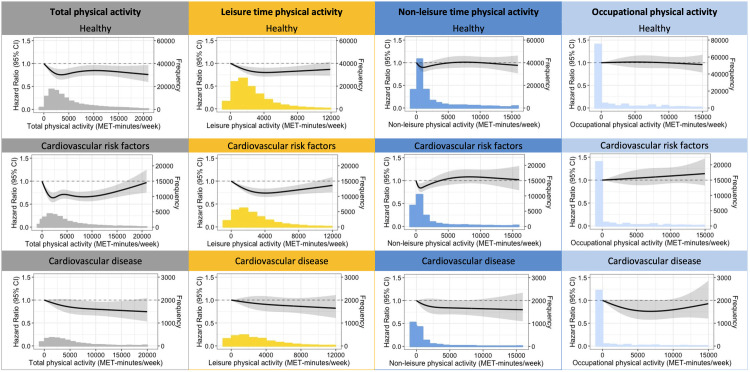
MVPA is beneficial for reducing adverse outcomes, but the shape of the association depends on cardiovascular health status. A curvilinear association was found in healthy and CVRF individuals with a steep risk reduction at low to moderate MVPA volumes and benefits plateauing at high(er) MVPA volumes. CVD patients demonstrated a linear association, suggesting a constant reduction of risk with higher volumes of MVPA. Therefore, individuals with CVDs should be encouraged that "more is better" regarding MVPA. These findings may help to optimize exercise prescription to gain maximal benefits of a physically active lifestyle.
中等到剧烈的身体活动(MVPA)与非传染性疾病和死亡率降低密切相关。心血管健康状况可能会影响 MVPA 的益处。我们比较了健康个体、心血管危险因素(CVRF)水平升高的个体和心血管疾病(CVD)个体之间,MVPA 与主要不良心血管事件(MACE)和死亡率的相关性。
在荷兰北部的 3 个省进行了一项队列研究,数据收集于 2006 年至 2018 年之间,中位随访时间为 6.8 年(Q25 为 5.7;Q75 为 7.9)。基线时,Lifelines 队列研究的 142493 名参与者分为(1)健康;(2)CVRF;或(3)CVD。根据自我报告的 MVPA 量,个体被分为“不活动”和最少(Q1)到最多(Q4)活跃的 4 个四分位数。主要结局是随访期间发生的 MACE 和全因死亡率的复合事件。使用 Cox 回归估计危险比(HRs)、95%置信区间(CIs)和 P 值。主要分析按基线健康状况分层,并调整了年龄、性别、收入、教育、饮酒、吸烟、蛋白质、脂肪和碳水化合物摄入、肾功能、心律失常、甲状腺功能减退、肺部疾病、骨关节炎和类风湿关节炎。健康个体的事件发生率为 2.2%(n = 2485 例,n = 112018 例),CVRF 个体为 7.9%(n = 2214 例,n = 27982 例),CVD 个体为 40.9%(n = 1019 例,n = 2493 例)。对于健康个体(P = 0.36)和 CVRF 个体(P = 0.86),MVPA 与全因死亡率或 MACE 之间没有线性关联,但对于 CVD 个体(P = 0.04)则存在线性关联。健康个体的调整后 HR 分别为 0.81(95%CI 0.64 至 1.02,P = 0.07)、0.71(95%CI 0.56 至 0.89,P = 0.004)、0.72(95%CI 0.57 至 0.91,P = 0.006)和 0.76(95%CI 0.60 至 0.96,P = 0.02),与不活动个体相比。在 CVRF 个体中,HR 分别为 0.69(95%CI 0.57 至 0.82,P < 0.001)、0.66(95%CI 0.55 至 0.80,P < 0.001)、0.64(95%CI 0.53 至 0.77,P < 0.001)和 0.69(95%CI 0.57 至 0.84,P < 0.001),与不活动个体相比。最后,与不活动个体相比,CVD 患者的 MVPA Q1 至 Q4 的 HR 分别为 0.80(95%CI 0.62 至 1.03,P = 0.09)、0.82(95%CI 0.63 至 1.06,P = 0.13)、0.74(95%CI 0.57 至 0.95,P = 0.02)和 0.70(95%CI 0.53 至 0.93,P = 0.01)。休闲时间的 MVPA 与最大的健康益处相关,非休闲时间的 MVPA 与很少的健康益处相关,而职业时间的 MVPA 与健康益处无关。研究的局限性包括其观察性性质、自我报告的 MVPA 数据以及尽管对生活方式风险因素和健康相关因素进行了广泛调整,但可能存在残余混杂。
MVPA 有益于降低不良后果,但关联的形状取决于心血管健康状况。在健康和 CVRF 个体中,发现了一种曲线关联,在低至中度 MVPA 量时,风险降低幅度陡峭,而在高(更高)MVPA 量时,效益趋于平稳。CVD 患者则表现出线性关联,表明随着 MVPA 量的增加,风险持续降低。因此,应该鼓励 CVD 患者,认为“越多越好”,多进行 MVPA。这些发现可能有助于优化运动处方,以获得积极生活方式的最大益处。