Monlezun Dominique J, Samura Alfred T, Patel Ritesh S, Thannoun Tariq E, Balan Prakash
Department of Cardiology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Center for Artificial Intelligence and Health Equities, Global System Analytics & Structures, Bethesda, MD, USA.
Cardiol Res Pract. 2021 Nov 24;2021:3180987. doi: 10.1155/2021/3180987. eCollection 2021.
Social disparities in out-of-hospital cardiac arrest (OHCA) outcomes are preventable, costly, and unjust. We sought to perform the first large artificial intelligence- (AI-) guided statistical and geographic information system (GIS) analysis of a multiyear and multisite cohort for OHCA outcomes (incidence and poor neurological disposition).
We conducted a retrospective cohort analysis of a prospectively collected multicenter dataset of adult patients who sequentially presented to Houston metro area hospitals from 01/01/07-01/01/16. Then AI-based machine learning (backward propagation neural network) augmented multivariable regression and GIS heat mapping were performed.
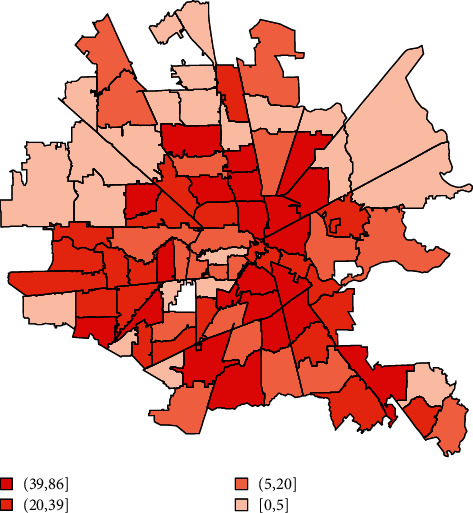
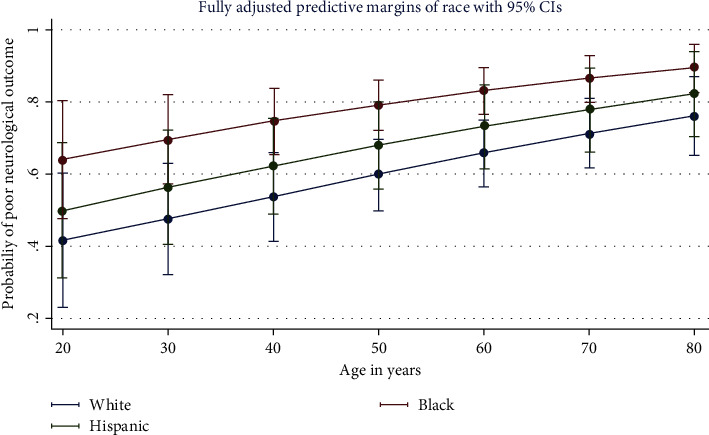
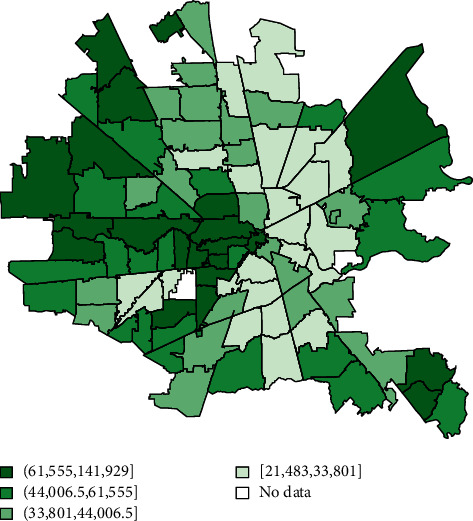
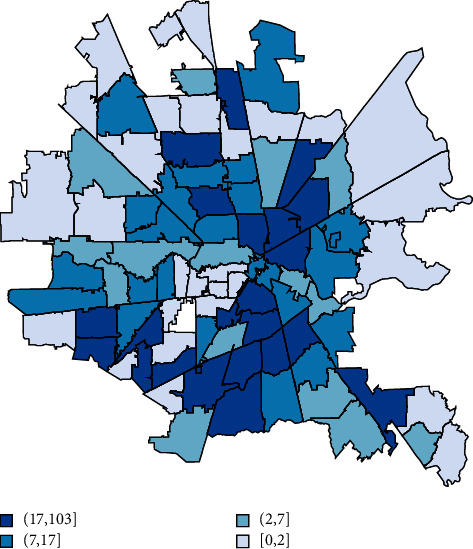
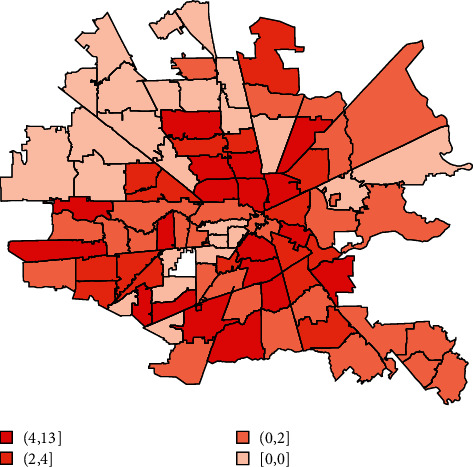
Of 3,952 OHCA patients across 38 hospitals, African Americans were the most likely to suffer OHCA despite representing a significantly lower percentage of the population (42.6 versus 22.8%; < 0.001). Compared to Caucasians, they were significantly more likely to have poor neurological disposition (OR 2.21, 95%CI 1.25-3.92; =0.006) and be discharged to a facility instead of home (OR 1.39, 95%CI 1.05-1.85; =0.023). Compared to the safety net hospital system primarily serving poorer African Americans, the university hospital serving primarily higher income commercially and Medicare insured patients had the lowest odds of death (OR 0.45, < 0.001). Each additional $10,000 above median household income was associated with a decrease in the total number of cardiac arrests per zip code by 2.86 (95%CI -4.26- -1.46; < 0.001); zip codes with a median income above $54,600 versus the federal poverty level had 14.62 fewer arrests ( < 0.001). GIS maps showed convergence of the greater density of poor neurologic outcome cases and greater density of poorer African American residences.
This large, longitudinal AI-guided analysis statistically and geographically identifies racial and socioeconomic disparities in OHCA outcomes in a way that may allow targeted medical and public health coordinated efforts to improve clinical, cost, and social equity outcomes.
院外心脏骤停(OHCA)结局中的社会差异是可预防的、代价高昂且不公平的。我们试图对一个多年多地点的OHCA结局(发病率和不良神经学转归)队列进行首次大规模人工智能(AI)引导的统计和地理信息系统(GIS)分析。
我们对一个前瞻性收集的多中心数据集进行了回顾性队列分析,该数据集包含2007年1月1日至2016年1月1日期间陆续就诊于休斯顿都会区医院的成年患者。然后进行了基于AI的机器学习(反向传播神经网络)增强多变量回归和GIS热图分析。
在38家医院的3952例OHCA患者中,非裔美国人尽管在总人口中所占比例显著较低(42.6%对22.8%;P<0.001),但却是最易发生OHCA的群体。与白种人相比,他们发生不良神经学转归的可能性显著更高(比值比[OR]2.21,95%置信区间[CI]1.25 - 3.92;P = 0.006),且出院后入住机构而非回家的可能性也更高(OR 1.39,95%CI 1.05 - 1.85;P = 0.023)。与主要服务贫困非裔美国人的安全网医院系统相比,主要服务高收入商业保险和医疗保险参保患者的大学医院死亡几率最低(OR 0.45,P<0.001)。家庭收入中位数每增加10,000美元,每个邮政编码区域的心脏骤停总数就减少2.86例(95%CI - 4.26至 - 1.46;P<0.001);家庭收入中位数高于54,600美元相对于联邦贫困线的邮政编码区域心脏骤停减少14.62例(P<0.001)。GIS地图显示不良神经学结局病例密度较高的区域与贫困非裔美国人居住密度较高的区域相互重叠。
这项大规模、纵向的AI引导分析从统计和地理角度识别了OHCA结局中的种族和社会经济差异,这可能有助于开展有针对性的医疗和公共卫生协同努力,以改善临床、成本和社会公平结局。