School of Public Health, Fudan University, Shanghai, 200433, China.
Key Lab of Health Technology Assessment, National Health Commission of the People's Republic of China, Shanghai, 200433, China.
Neurosurg Rev. 2022 Apr;45(2):1291-1302. doi: 10.1007/s10143-021-01704-0. Epub 2021 Dec 6.
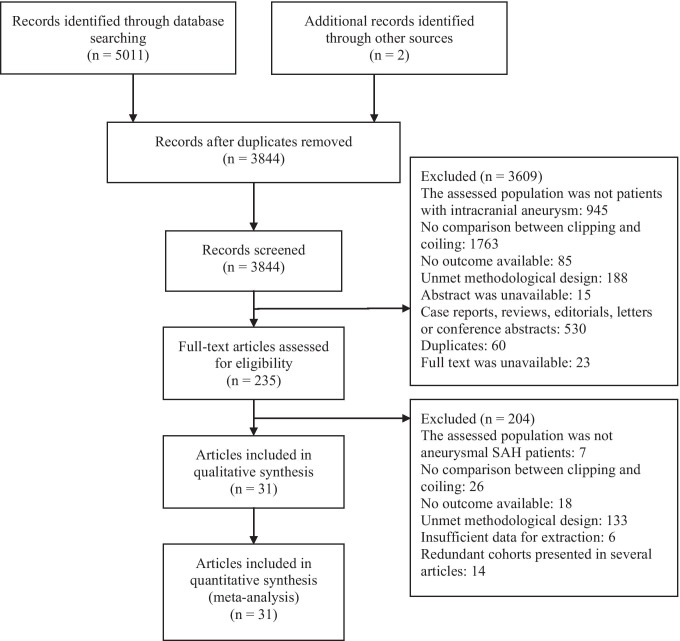
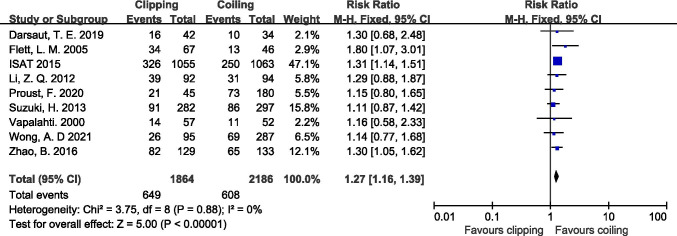
Neurosurgical clipping and endovascular coiling are both standard therapies to prevent rebleeding after aneurysmal subarachnoid hemorrhage (aSAH). However, controversy still exists about which is the optimal treatment. This meta-analysis aims to assess the effectiveness and safety of two treatments with high-quality evidence. Web of Science, Cochrane Library, EMBASE, Pubmed, Sinomed, China National Knowledge Infrastructure, and Wanfang Data databases were systematically searched on August 5, 2021. Randomized controlled trials (RCTs) and prospective cohort studies that evaluated the effectiveness and safety of clipping versus coiling in aSAH patients at discharge or within 1-year follow-up period were eligible. No restriction was set on the publication date. Meta-analyses were conducted to calculate the pooled estimates and 95% confidence intervals (CI) of relative risk (RR). Eight RCTs and 20 prospective cohort studies were identified. Compared to coiling, clipping was associated with a lower rebleeding rate at discharge (RR: 0.52, 95% CI: 0.29--0.94) and a higher aneurysmal occlusion rate (RR: 1.33, 95% CI: 1.19-1.48) at 1-year follow-up. In contrast, coiling reduced the vasospasm rate at discharge (RR: 1.45, 95% CI: 1.23-1.71) and 1-year poor outcome rate (RR: 1.27, 95% CI: 1.16-1.39). Subgroup analyses presented that among patients with a poor neurological condition at admission, no statistically significant outcome difference existed between the two treatments. The overall prognosis was better among patients who received coiling, but this advantage was not significant among patients with a poor neurological condition at admission. Therefore, the selection of treatment modality for aSAH patients should be considered comprehensively.
神经外科夹闭术和血管内介入栓塞术都是预防蛛网膜下腔出血(aSAH)后再出血的标准治疗方法。然而,哪种治疗方法更优仍存在争议。本荟萃分析旨在使用高质量证据评估这两种治疗方法的有效性和安全性。于 2021 年 8 月 5 日,系统地检索了 Web of Science、Cochrane 图书馆、EMBASE、Pubmed、中国生物医学文献数据库、中国知网和万方数据资源系统。纳入评估夹闭术与血管内介入栓塞术在出院或 1 年随访期 aSAH 患者中的有效性和安全性的随机对照试验(RCT)和前瞻性队列研究。未对发表日期进行限制。采用荟萃分析计算相对风险(RR)的合并估计值和 95%置信区间(CI)。共纳入 8 项 RCT 和 20 项前瞻性队列研究。与血管内介入栓塞术相比,夹闭术在出院时的再出血率(RR:0.52,95%CI:0.29--0.94)和 1 年时的动脉瘤闭塞率(RR:1.33,95%CI:1.19-1.48)较低。相反,血管内介入栓塞术降低了出院时(RR:1.45,95%CI:1.23-1.71)和 1 年时不良结局发生率(RR:1.27,95%CI:1.16-1.39)。亚组分析表明,在入院时神经功能状态较差的患者中,两种治疗方法之间没有统计学显著的结局差异。血管内介入栓塞术治疗的患者总体预后较好,但在入院时神经功能状态较差的患者中,这种优势并不显著。因此,应综合考虑 aSAH 患者的治疗方式选择。