Na Soo Jin, Ko Ryoung-Eun, Ko Myeong Gyun, Jeon Kyeongman
Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea.
Intensive Care Unit Nursing Department, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea.
J Intensive Care. 2021 Dec 7;9(1):73. doi: 10.1186/s40560-021-00588-y.
Timely recognition of warning signs from deteriorating patients and proper treatment are important in improving patient safety. In comparison to the traditional medical emergency team (MET) activation triggered by phone calls, automated activation of MET may minimize activation delays. However, limited data are available on the effects of automated activation systems on the time from derangement to MET activation and on clinical outcomes. The objective of this study was to determine the impact of an automated alert and activation system for MET on clinical outcomes in unselected hospitalized patients.
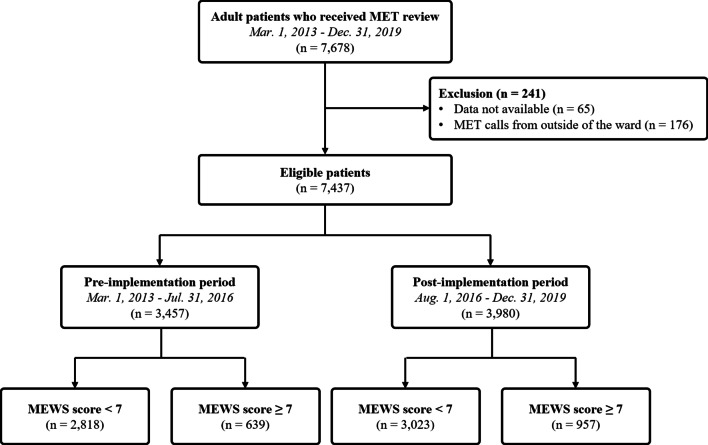
This is an observational study using prospectively collected data from consecutive patients managed by the MET at a university-affiliated, tertiary hospital from March 2013 to December 2019. The automated alert system automatically calculates the Modified Early Warning Score (MEWS) and subsequently activates MET when the MEWS score is 7 or higher, which was implemented since August 2016. The outcome measures of interest including hospital mortality in patients with MEWS of 7 or higher were compared between pre-implementation and post-implementation groups of the automated alert and activation system in the primary analysis. The association between the implementation of the system and hospital mortality was evaluated with logistic regression analysis.
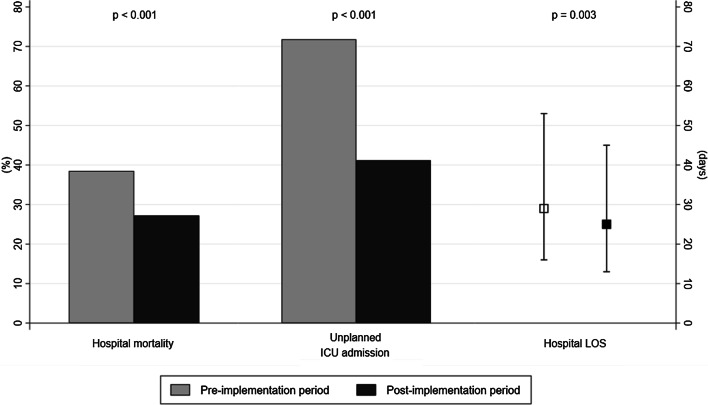
Of the 7678 patients who were managed by MET during the study period, 639 patients during the pre-implementation period and 957 patients during the post-implementation period were included in the primary analysis. MET calls due to abnormal physiological variables were more common during the pre-implementation period, while MET calls due to medical staff's worries or concern about the patient's condition were more common during the post-implementation period. The median time from deterioration to MET activation was significantly shortened in the post-implementation period compared to the pre-implementation period (34 min vs. 60 min, P < 0.001). In addition, unplanned ICU admission rates (41.2% vs. 71.8%, P < 0.001) was reduced during the post-implementation period. Hospital mortality was decreased after implementation of the automated alert system (27.2% vs. 38.5%, P < 0.001). The implementation of the automated alert and activation system was associated with decreased risk of death in the multivariable analysis (adjusted OR 0.73, 95% CI 0.56-0.90).
After implementing an automated alert and activation system, the time from deterioration to MET activation was shortened and clinical outcomes were improved in hospitalized patients.
及时识别病情恶化患者的警示信号并进行恰当治疗对于提高患者安全至关重要。与传统的通过电话触发的医疗急救团队(MET)启动相比,MET的自动启动可能会最大程度地减少启动延迟。然而,关于自动启动系统对从病情紊乱到MET启动的时间以及临床结局影响的数据有限。本研究的目的是确定MET自动警报和启动系统对未选定的住院患者临床结局的影响。
这是一项观察性研究,使用了2013年3月至2019年12月在一家大学附属医院由MET管理的连续患者的前瞻性收集数据。自动警报系统会自动计算改良早期预警评分(MEWS),当MEWS评分达到7或更高时会随后启动MET,该系统自2016年8月起实施。在主要分析中,比较了自动警报和启动系统实施前和实施后组中MEWS为7或更高的患者的包括医院死亡率在内的感兴趣的结局指标。通过逻辑回归分析评估系统实施与医院死亡率之间的关联。
在研究期间由MET管理的7678例患者中,主要分析纳入了实施前时期的639例患者和实施后时期的957例患者。在实施前时期,因生理变量异常导致的MET呼叫更为常见,而在实施后时期,因医护人员对患者病情的担忧导致的MET呼叫更为常见。与实施前时期相比,实施后时期从病情恶化到MET启动的中位时间显著缩短(34分钟对60分钟,P<0.001)。此外,实施后时期非计划入住重症监护病房的比率降低(41.2%对71.8%,P<0.001)。实施自动警报系统后医院死亡率降低(27.2%对38.5%,P<0.001)。在多变量分析中,自动警报和启动系统的实施与死亡风险降低相关(调整后的比值比为0.73,95%置信区间为0.56-0.90)。
实施自动警报和启动系统后,住院患者从病情恶化到MET启动的时间缩短,临床结局得到改善。