Hartford Luke B, Allen Laura J, Lennox Heather, Jairath Vipul, Van Koughnett Julie Ann M
Division of General Surgery, Department of Surgery, Schulich School of Medicine and Dentistry, Western University, General Surgery, London Health Science Centre, London, Ontario, Canada.
Division of Gastroenterology, Department of Medicine, Schulich School of Medicine and Dentistry, Western University, London Health Sciences Centre, London, Ontario, Canada.
J Can Assoc Gastroenterol. 2021 May 8;4(6):284-289. doi: 10.1093/jcag/gwab004. eCollection 2021 Dec.
Multidisciplinary conference presentation may provide recommendations for diagnosis, monitoring and treatment for patients with inflammatory bowel disease.
A prospective observational study was completed evaluating if case presentation resulted in a direct change in management for patients presented over a 2-year period in a tertiary Canadian centre. Change in management was defined as hospital admission, surgery or surgical referral, start/change in biologic therapy or other medication or initiation of parenteral nutrition. Secondary outcomes included the involvement of specialists and other referrals. Data were analyzed using frequencies and means with standard deviations.
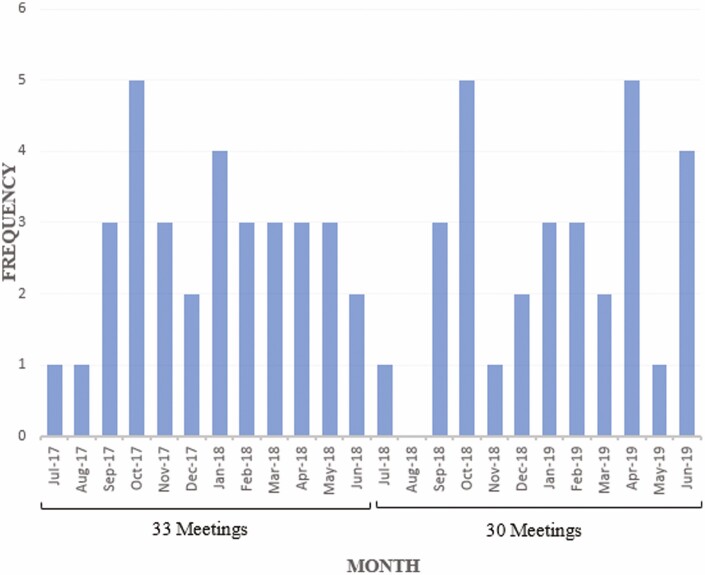
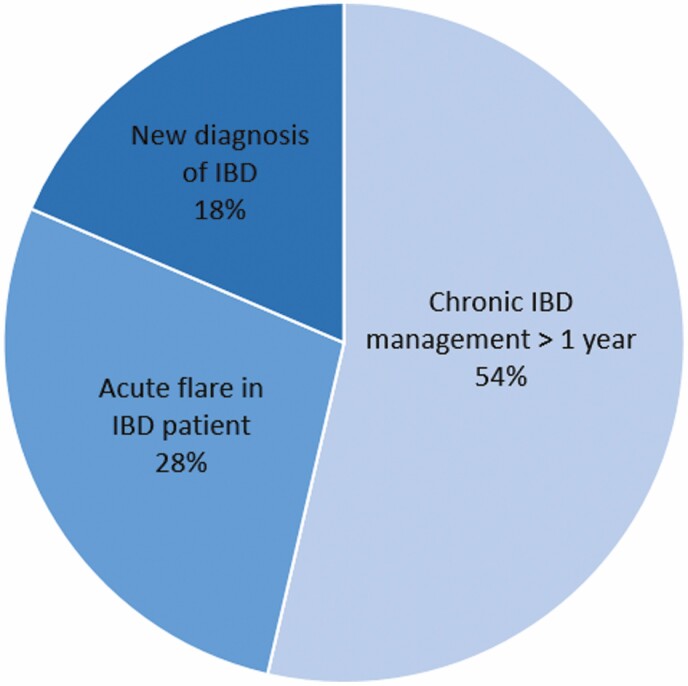
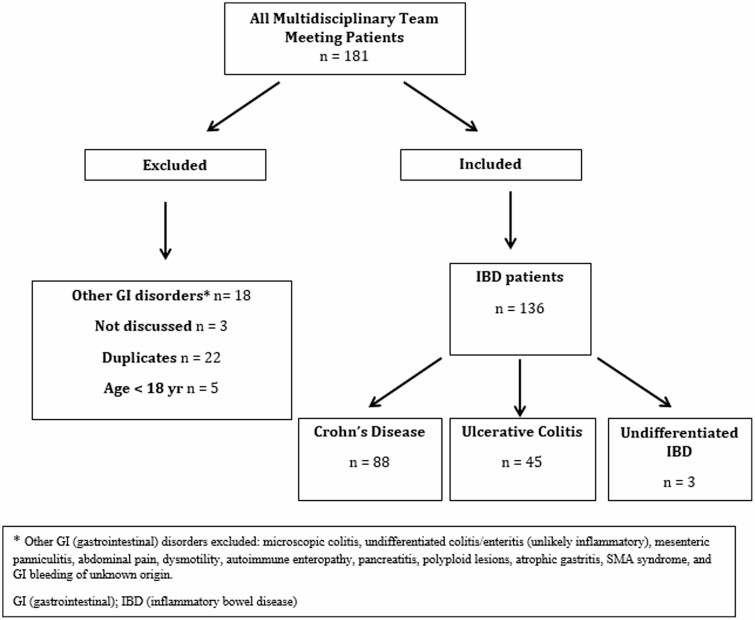
In 63 multidisciplinary conferences, 181 patients were presented, of whom 136 patients met the inclusion criteria of inflammatory bowel disease (Crohn's = 45, ulcerative colitis = 88, undifferentiated = 3). The majority were outpatient cases 110 (81%). Indications included 71 (52%) patients presented for IBD management with diagnosis > 1 year, 37 (27%) with an acute IBD flare in a chronic patient (>1 year since diagnosis) and 24 (18%) with new diagnosis of IBD. Change in management was recommended in 35 (26%) patients. The most common change was referral to surgery in 17 (13%), surgery in 12 (9%) or change in biologic therapy 11 (8%). Compliance with the recommendations was 85%. There was frequent specialist involvement in case discussions (gastroenterologist 100%, surgeon 60%, radiologist 68% and pathologist 32%).
Presentation of complex inflammatory bowel disease cases at multidisciplinary conference leads to a direct change in treatment in one quarter of cases, with surgical referral as the most frequent outcome.
多学科会议报告可为炎症性肠病患者的诊断、监测和治疗提供建议。
完成了一项前瞻性观察性研究,评估病例报告是否会导致加拿大一家三级中心在两年期间所报告患者的管理发生直接变化。管理变化定义为住院、手术或手术转诊、生物治疗或其他药物的开始/改变或肠外营养的启动。次要结果包括专科医生的参与和其他转诊情况。使用频率和均值以及标准差对数据进行分析。
在63次多学科会议上,报告了181例患者,其中136例患者符合炎症性肠病的纳入标准(克罗恩病 = 45例,溃疡性结肠炎 = 88例,未分化型 = 3例)。大多数为门诊病例110例(81%)。报告指征包括71例(52%)因炎症性肠病管理前来就诊且诊断时间>1年的患者,37例(27%)慢性患者(诊断后>1年)出现急性炎症性肠病发作的患者以及24例(18%)新诊断为炎症性肠病的患者。35例(26%)患者的管理建议发生了变化。最常见的变化是17例(13%)转诊至外科手术、12例(9%)进行手术或11例(8%)改变生物治疗。对建议的依从率为85%。病例讨论中经常有专科医生参与(胃肠病学家参与率100%,外科医生参与率60%,放射科医生参与率68%,病理科医生参与率32%)。
在多学科会议上展示复杂的炎症性肠病病例会导致四分之一的病例治疗发生直接变化,手术转诊是最常见的结果。