Sharkey Amy R, Sah Bert-Ram, Withey Samuel J, Bhuva Shaheel, Neji Radhouene, Jeljeli Sami, Green Adrian, Cook Gary J R, Goh Vicky
Department of Cancer Imaging, School of Biomedical Engineering and Imaging Sciences, King's College London, London, UK.
Department of Radiology, Guy's and St Thomas' NHS Foundation Trust, London, UK.
Eur J Hybrid Imaging. 2021 Dec 13;5(1):23. doi: 10.1186/s41824-021-00117-y.
F-fluorodeoxyglucose positron emission tomography/magnetic resonance imaging (18F-FDG PET/MRI) may improve cancer staging by combining sensitive cancer detection with high-contrast resolution and detail. We compared the diagnostic performance of 18F-FDG PET/MRI to F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) for staging oesophageal/gastro-oesophageal cancer. Following ethical approval and informed consent, participants with newly diagnosed primary oesophageal/gastro-oesophageal cancer were enrolled. Exclusions included prior/concurrent malignancy. Following 324 ± 28 MBq 18F-FDG administration and 60-min uptake, PET/CT was performed, immediately followed by integrated PET/MRI from skull base to mid-thigh. PET/CT was interpreted by two dual-accredited nuclear medicine physicians and PET/MRI by a dual-accredited nuclear medicine physician/radiologist and cancer radiologist in consensus. Per-participant staging was compared with the tumour board consensus staging using the McNemar test, with statistical significance at 5%.
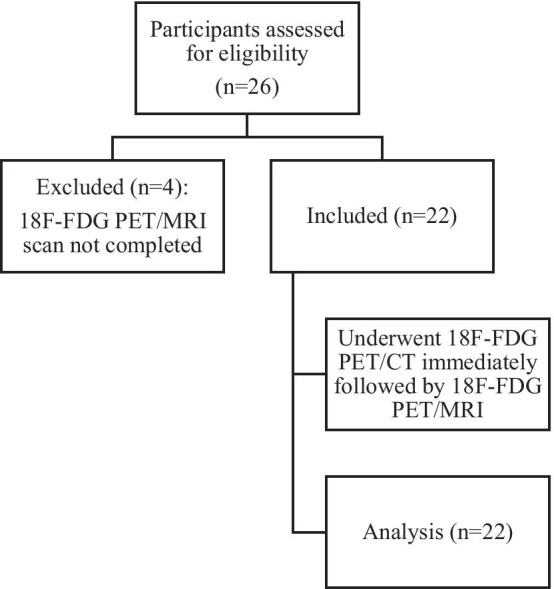
Out of 26 participants, 22 (20 males; mean ± SD age 68.8 ± 8.7 years) completed 18F-FDG PET/CT and PET/MRI. Compared to the tumour board, the primary tumour was staged concordantly in 55% (12/22) with PET/MRI and 36% (8/22) with PET/CT; the nodal stage was concordant in 45% (10/22) with PET/MRI and 50% (11/22) with PET/CT. There was no statistical difference in PET/CT and PET/MRI staging performance (p > 0.05, for T and N staging). The staging of distant metastases was concordant with the tumour board in 95% (21/22) with both PET/MRI and PET/CT. Of participants with distant metastatic disease, PET/MRI detected additional metastases in 30% (3/10).
In this preliminary study, compared to 18F-FDG PET/CT, 18F-FDG PET/MRI showed non-significant higher concordance with T-staging, but no difference with N or M-staging. Additional metastases detected by 18F-FDG PET/MRI may be of additive clinical value.
氟脱氧葡萄糖正电子发射断层扫描/磁共振成像(18F-FDG PET/MRI)可通过将灵敏的癌症检测与高对比度分辨率及细节相结合来改善癌症分期。我们比较了18F-FDG PET/MRI与氟脱氧葡萄糖正电子发射断层扫描/计算机断层扫描(18F-FDG PET/CT)对食管癌/胃食管癌进行分期的诊断性能。在获得伦理批准并取得知情同意后,纳入新诊断的原发性食管癌/胃食管癌患者。排除标准包括既往/同时存在的恶性肿瘤。静脉注射324±28 MBq 18F-FDG并经过60分钟摄取后,进行PET/CT检查,随后立即进行从头颅底部至大腿中部的PET/MRI联合检查。PET/CT由两名具有双重资质的核医学医师解读,PET/MRI由一名具有双重资质的核医学医师/放射科医师和一名癌症放射科医师共同解读并达成共识。使用McNemar检验将每位参与者的分期与肿瘤委员会的共识分期进行比较,以5%作为统计学显著性水平。
26名参与者中,22名(20名男性;平均±标准差年龄68.8±8.7岁)完成了18F-FDG PET/CT和PET/MRI检查。与肿瘤委员会的分期相比,PET/MRI对原发肿瘤分期的一致性为55%(12/22),PET/CT为36%(8/22);PET/MRI对区域淋巴结分期的一致性为45%(10/22),PET/CT为50%(11/22)。PET/CT和PET/MRI的分期性能无统计学差异(T分期和N分期的p>0.05)。PET/MRI和PET/CT对远处转移分期与肿瘤委员会的一致性均为95%(21/22)。在有远处转移的参与者中,PET/MRI额外检测到30%(3/10)的转移灶。
在这项初步研究中,与18F-FDG PET/CT相比,18F-FDG PET/MRI在T分期方面显示出非显著性更高的一致性,但在N分期或M分期方面无差异。18F-FDG PET/MRI检测到的额外转移灶可能具有附加临床价值。