Prevent Breast Cancer Research Unit, The Nightingale Centre, Manchester University NHS Foundation Trust, Manchester, England.
Division of Cancer Sciences, The University of Manchester, Manchester, England.
Br J Cancer. 2022 May;126(8):1157-1167. doi: 10.1038/s41416-021-01650-0. Epub 2021 Dec 15.
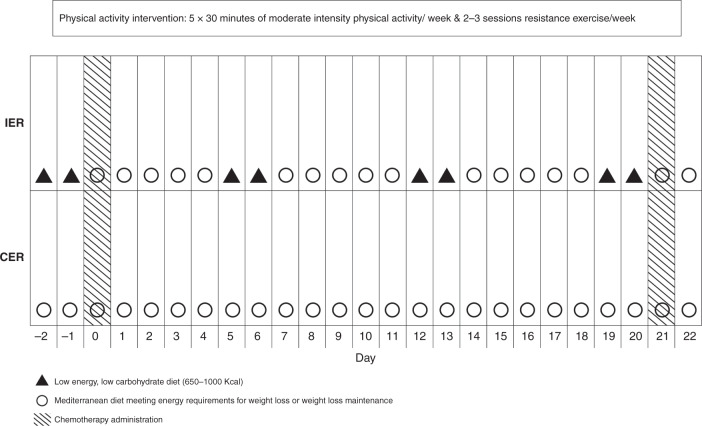
Excess adiposity at diagnosis and weight gain during chemotherapy is associated with tumour recurrence and chemotherapy toxicity. We assessed the efficacy of intermittent energy restriction (IER) vs continuous energy restriction (CER) for weight control and toxicity reduction during chemotherapy.
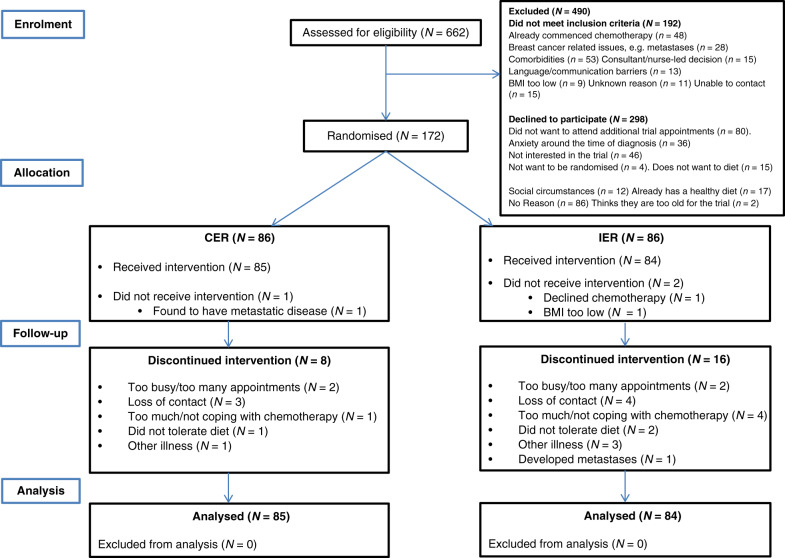
One hundred and seventy-two women were randomised to follow IER or CER throughout adjuvant/neoadjuvant chemotherapy. Primary endpoints were weight and body fat change. Secondary endpoints included chemotherapy toxicity, cardiovascular risk markers, and correlative markers of metabolism, inflammation and oxidative stress.
Primary analyses showed non-significant reductions in weight (-1.1 (-2.4 to +0.2) kg, p = 0.11) and body fat (-1.0 (-2.1 to +0.1) kg, p = 0.086) in IER compared with CER. Predefined secondary analyses adjusted for body water showed significantly greater reductions in weight (-1.4 (-2.5 to -0.2) kg, p = 0.024) and body fat (-1.1 (-2.1 to -0.2) kg, p = 0.046) in IER compared with CER. Incidence of grade 3/4 toxicities were comparable overall (IER 31.0 vs CER 36.5%, p = 0.45) with a trend to fewer grade 3/4 toxicities with IER (18%) vs CER (31%) during cycles 4-6 of primarily taxane therapy (p = 0.063).
IER is feasible during chemotherapy. The potential efficacy for weight control and reducing toxicity needs to be tested in future larger trials.
ISRCTN04156504.
诊断时的超重和化疗期间的体重增加与肿瘤复发和化疗毒性有关。我们评估了间歇能量限制(IER)与连续能量限制(CER)在化疗期间控制体重和减少毒性的效果。
172 名女性被随机分配在辅助/新辅助化疗期间遵循 IER 或 CER。主要终点是体重和体脂变化。次要终点包括化疗毒性、心血管风险标志物以及代谢、炎症和氧化应激的相关标志物。
主要分析显示,IER 组与 CER 组相比,体重(-1.1(-2.4 至 +0.2)kg,p=0.11)和体脂(-1.0(-2.1 至 +0.1)kg,p=0.086)的减轻无显著差异。针对身体水分进行的预先定义的二次分析显示,IER 组体重(-1.4(-2.5 至 -0.2)kg,p=0.024)和体脂(-1.1(-2.1 至 -0.2)kg,p=0.046)的减轻显著更大。总体而言,3/4 级毒性的发生率相当(IER 31.0%与 CER 36.5%,p=0.45),IER(18%)在主要紫杉醇治疗的第 4-6 个周期中比 CER(31%)的 3/4 级毒性发生率趋势更低(p=0.063)。
IER 在化疗期间是可行的。在未来更大的试验中,需要测试其控制体重和减少毒性的潜在效果。
ISRCTN04156504。