Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland.
Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland; Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, Maryland; Center for Drug Safety and Effectiveness, Johns Hopkins University, Baltimore, Maryland; Welch Center for Prevention, Epidemiology and Clinical Research, Johns Hopkins University, Baltimore, Maryland.
Am J Cardiol. 2022 Feb 15;165:124-130. doi: 10.1016/j.amjcard.2021.11.013. Epub 2021 Dec 20.
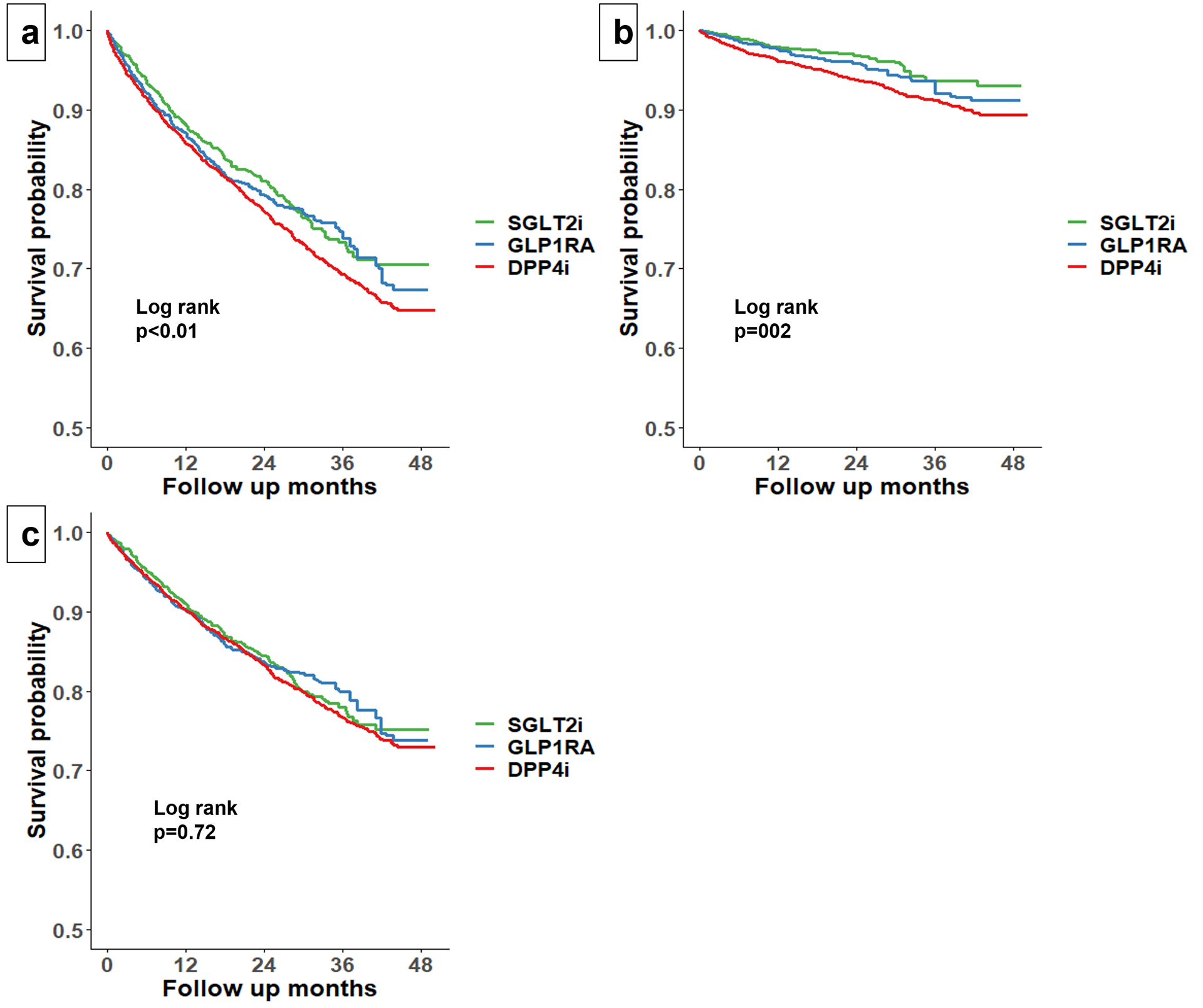
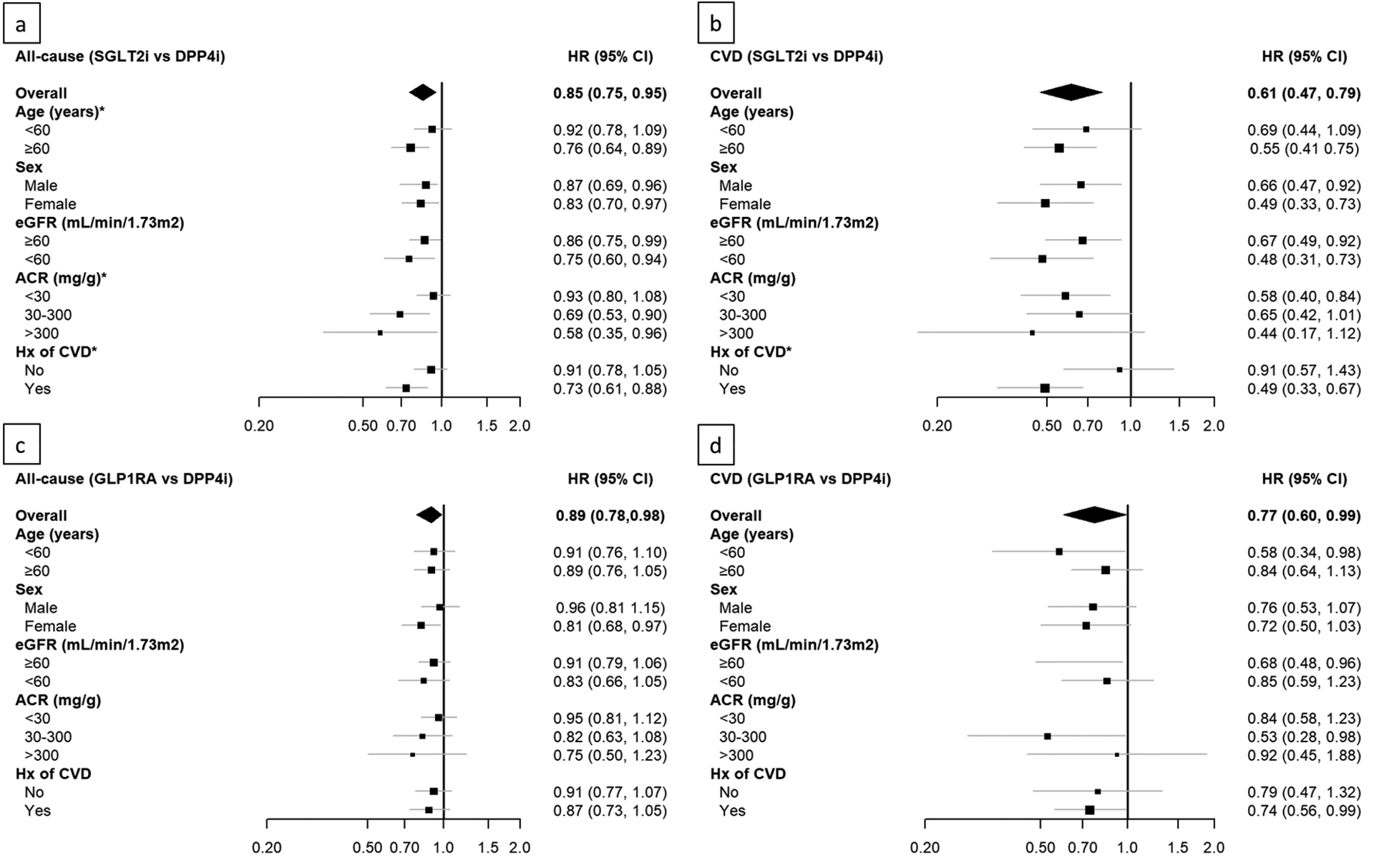
Clinical trials have demonstrated cardiovascular benefits of sodium-glucose cotransporter 2 inhibitors (SGLT2i) and glucagon-like peptide-1 receptor agonists (GLP-1RA). However, their impact on all-cause and cause-specific hospitalization in real-world practice remains unclear. We identified patients with diabetes who initiated SGLT2i (n = 2,492), GLP-1RA (n = 1,982), or dipeptidyl peptidase-4 inhibitors (DPP4i, n = 2,492) between 2015 and 2018 in Geisinger Health System. We examined all-cause hospitalization (net benefit indicator) and cardiovascular disease (CVD) hospitalization (CV benefit indicator), as well as non-CVD hospitalization (harm indicator), using Cox proportional hazards regression. During a median follow-up of 16 months, SGLT2i and GLP-1RA were associated with lower risk of all-cause hospitalization (hazard ratio [HR] 0.85, 95% CI 0.75 to 0.95 for SGLT2i; HR 0.89, 95% CI 0.78 to 0.98 for GLP-1RA), as well as CVD hospitalization (HR 0.61, 95% CI 0.47 to 0.79) for SGLT2i; HR 0.77, 95% CI 0.60 to 0.99 for GLP-1RA) compared with DPP4i. The risks of all-cause and CVD hospitalization were similar between SGLT2i and GLP-1RA. SGLT2i was associated with substantially lower risk of myocardial infarction and heart failure hospitalization compared with DPP4i and lower risk of heart failure hospitalization compared with GLP-1RA. The risk of non-CVD hospitalization did not differ among the treatment groups. These results from real-world comparison further encourage SGLT2i and GLP-1RA use in routine diabetes care, particularly among patients at high risk of cardiovascular events.
临床试验已经证明钠-葡萄糖共转运蛋白 2 抑制剂(SGLT2i)和胰高血糖素样肽-1 受体激动剂(GLP-1RA)对心血管有获益。然而,它们在真实世界实践中对全因和特定病因住院的影响仍不清楚。我们在 Geisinger 健康系统中确定了 2015 年至 2018 年间开始使用 SGLT2i(n=2492)、GLP-1RA(n=1982)或二肽基肽酶-4 抑制剂(DPP4i,n=2492)的糖尿病患者。我们使用 Cox 比例风险回归检查了全因住院(净获益指标)和心血管疾病(CVD)住院(CV 获益指标)以及非 CVD 住院(危害指标)。在中位随访 16 个月期间,SGLT2i 和 GLP-1RA 与全因住院风险降低相关(SGLT2i 的危险比[HR]0.85,95%CI0.75 至 0.95;GLP-1RA 的 HR0.89,95%CI0.78 至 0.98),SGLT2i 与 CVD 住院风险降低相关(HR0.61,95%CI0.47 至 0.79);GLP-1RA 的 HR0.77,95%CI0.60 至 0.99)相比,DPP4i。SGLT2i 和 GLP-1RA 之间的全因和 CVD 住院风险相似。SGLT2i 与 DPP4i 相比,心肌梗死和心力衰竭住院的风险显著降低,与 GLP-1RA 相比,心力衰竭住院的风险也降低。各组之间的非 CVD 住院风险没有差异。这些来自真实世界比较的结果进一步鼓励在常规糖尿病治疗中使用 SGLT2i 和 GLP-1RA,特别是在心血管事件风险较高的患者中。