Sait Afrah S, Chiang Teresa Po-Yu, Marr Kieren A, Massie Allan B, Cochran Willa, Shah Pali, Brennan Daniel C, Thomas Alvin G, Mehta Steinke Seema, Permpalung Nitipong, Shoham Shmuel, Merlo Christian, Jain Tania, Boyarsky Brian, Charnaya Olga, Gurakar Ahmet, Sharma Kavita, Durand Christine M, Werbel William A, Huang Chiung-Yu, Ostrander Darin, Desai Niraj, Kim Min Young, Alasfar Sami, Bloch Evan M, Tobian Aaron A R, Garonzik-Wang Jacqueline, Segev Dorry L, Avery Robin K
Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD.
Department of Surgery, Johns Hopkins University School of Medicine, Baltimore, MD.
Transplant Direct. 2021 Dec 23;8(1):e1268. doi: 10.1097/TXD.0000000000001268. eCollection 2022 Jan.
Few reports have focused on newer coronavirus disease 2019 (COVID-19) therapies (remdesivir, dexamethasone, and convalescent plasma) in solid organ transplant recipients; concerns had been raised regarding possible adverse impact on allograft function or secondary infections.
We studied 77 solid organ transplant inpatients with COVID-19 during 2 therapeutic eras (Era 1: March-May 2020, 21 patients; and Era 2: June-November 2020, 56 patients) and 52 solid organ transplant outpatients.
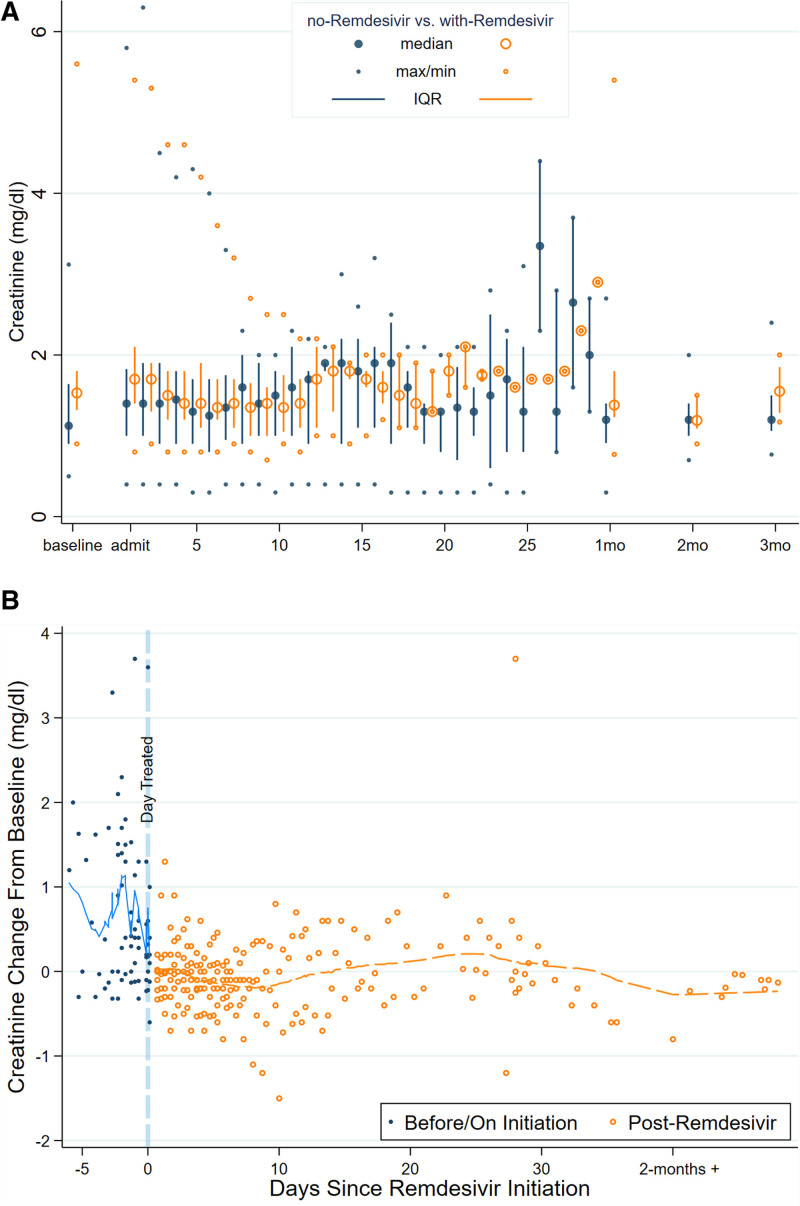
In Era 1, no patients received remdesivir or dexamethasone, and 4 of 21 (19.4%) received convalescent plasma, whereas in Era 2, remdesivir (24/56, 42.9%), dexamethasone (24/56, 42.9%), and convalescent plasma (40/56, 71.4%) were commonly used. Mortality was low across both eras, 4 of 77 (5.6%), and rejection occurred in only 2 of 77 (2.8%) inpatients; infections were similar in hypoxemic patients with or without dexamethasone. Preexisting graft dysfunction was associated with greater need for hospitalization, higher severity score, and lower survival. Acute kidney injury was present in 37.3% of inpatients; renal function improved more rapidly in patients who received remdesivir and convalescent plasma. Post-COVID-19 renal and liver function were comparable between eras, out to 90 d.
Newer COVID-19 therapies did not appear to have a deleterious effect on allograft function, and infectious complications were comparable.
很少有报告关注新型冠状病毒肺炎(COVID-19)的新型疗法(瑞德西韦、地塞米松和康复期血浆)在实体器官移植受者中的应用;人们对这些疗法可能对移植器官功能或继发感染产生的不利影响表示担忧。
我们研究了77例COVID-19实体器官移植住院患者,分两个治疗阶段(阶段1:2020年3月至5月,21例患者;阶段2:2020年6月至11月,56例患者),以及52例实体器官移植门诊患者。
在阶段1,没有患者接受瑞德西韦或地塞米松治疗,21例中有4例(19.4%)接受了康复期血浆治疗;而在阶段2,瑞德西韦(24/56,42.9%)、地塞米松(24/56,42.9%)和康复期血浆(40/56,71.4%)被普遍使用。两个阶段的死亡率都很低,77例中有4例(5.6%),住院患者中只有77例中的2例(2.8%)发生了排斥反应;使用或未使用地塞米松的低氧血症患者感染情况相似。移植前存在的移植物功能障碍与更高的住院需求、更高的严重程度评分和更低的生存率相关。37.3%的住院患者出现急性肾损伤;接受瑞德西韦和康复期血浆治疗的患者肾功能改善更快。两个阶段的COVID-19后肾和肝功能在90天内相当。
新型COVID-19疗法似乎对移植器官功能没有有害影响,且感染并发症相当。