Social, Genetic and Developmental Psychiatry Centre, Institute of Psychiatry, Psychology & Neuroscience, King's College London, Memory Lane, London, SE5 8AF, UK.
Department of Medical and Molecular Genetics, Faculty of Life Sciences & Medicine, King's College London, London, UK.
Sci Rep. 2022 Jan 10;12(1):459. doi: 10.1038/s41598-021-04016-x.
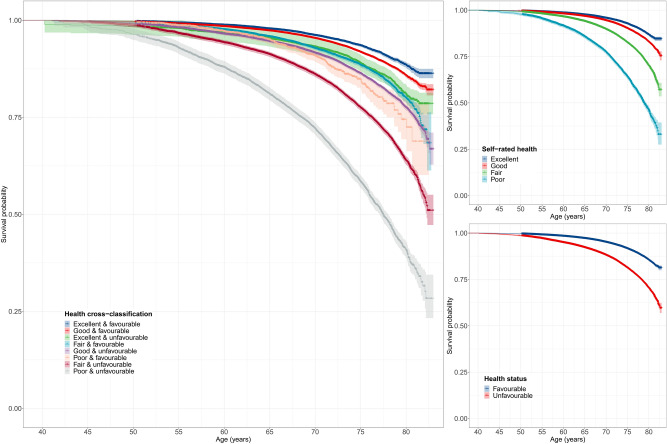
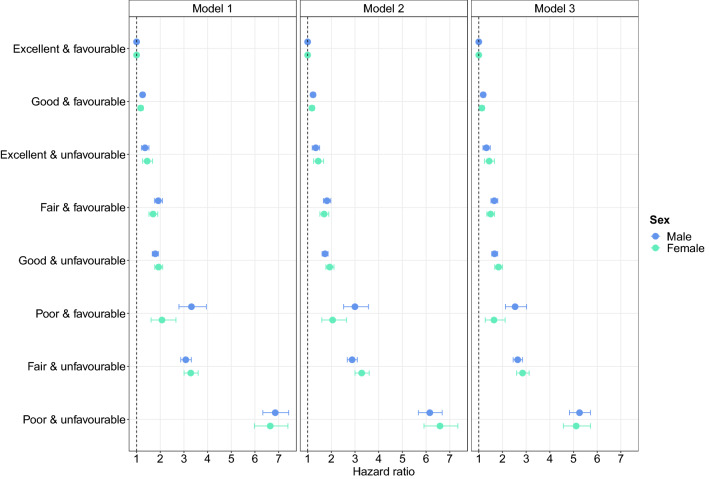
Risk stratification is an important public health priority that is central to clinical decision making and resource allocation. The aim of this study was to examine how different combinations of self-rated and objective health status predict all-cause mortality and leading causes of death in the UK. The UK Biobank study recruited > 500,000 participants between 2006 and 2010. Self-rated health was assessed using a single-item question and health status was derived from medical history, including data on 81 cancer and 443 non-cancer illnesses. Analyses included > 370,000 middle-aged and older adults with a median follow-up of 11.75 (IQR = 1.4) years, yielding 4,320,270 person-years of follow-up. Compared to individuals with excellent self-rated health and favourable health status, individuals with other combinations of self-rated and objective health status had a greater mortality risk, with hazard ratios ranging from HR = 1.22 (95% CI 1.15-1.29, P < 0.001) for individuals with good self-rated health and favourable health status to HR = 7.14 (95% CI 6.70-7.60, P < 0.001) for individuals with poor self-rated health and unfavourable health status. Our findings highlight that self-rated health captures additional health-related information and should be more widely assessed. The cross-classification between self-rated health and health status represents a straightforward metric for risk stratification, with applications to population health, clinical decision making and resource allocation.
风险分层是公共卫生的一个重要优先事项,是临床决策和资源分配的核心。本研究旨在探讨自我评估和客观健康状况的不同组合如何预测英国全因死亡率和主要死因。英国生物库研究于 2006 年至 2010 年期间招募了超过 50 万名参与者。自我评估健康状况采用单项问题进行评估,健康状况源自病史,包括 81 种癌症和 443 种非癌症疾病的数据。分析包括超过 37 万名中老年人,中位随访时间为 11.75 年(IQR=1.4),随访时间为 4320270 人年。与自我评估健康状况和健康状况良好的个体相比,自我评估和客观健康状况不同组合的个体具有更高的死亡率风险,风险比范围从自我评估健康状况良好和健康状况良好的个体的 HR=1.22(95%CI 1.15-1.29,P<0.001)到自我评估健康状况差和健康状况差的个体的 HR=7.14(95%CI 6.70-7.60,P<0.001)。我们的研究结果强调,自我评估健康状况可以捕捉到更多与健康相关的信息,应该更广泛地评估。自我评估健康状况和健康状况之间的交叉分类代表了一种简单的风险分层指标,适用于人群健康、临床决策和资源分配。