Center for Genomic Medicine, Massachusetts General Hospital and Harvard Medical School, Boston, MA, USA.
Broad Institute, Cambridge, MA, USA.
BMC Med. 2022 Jan 12;20(1):5. doi: 10.1186/s12916-021-02198-9.
Genetic and lifestyle factors have considerable effects on obesity and related diseases, yet their effects in a clinical cohort are unknown. This study in a patient biobank examined associations of a BMI polygenic risk score (PRS), and its interactions with lifestyle risk factors, with clinically measured BMI and clinical phenotypes.
The Mass General Brigham (MGB) Biobank is a hospital-based cohort with electronic health record, genetic, and lifestyle data. A PRS for obesity was generated using 97 genetic variants for BMI. An obesity lifestyle risk index using survey responses to obesogenic lifestyle risk factors (alcohol, education, exercise, sleep, smoking, and shift work) was used to dichotomize the cohort into high and low obesogenic index based on the population median. Height and weight were measured at a clinical visit. Multivariable linear cross-sectional associations of the PRS with BMI and interactions with the obesity lifestyle risk index were conducted. In phenome-wide association analyses (PheWAS), similar logistic models were conducted for 675 disease outcomes derived from billing codes.
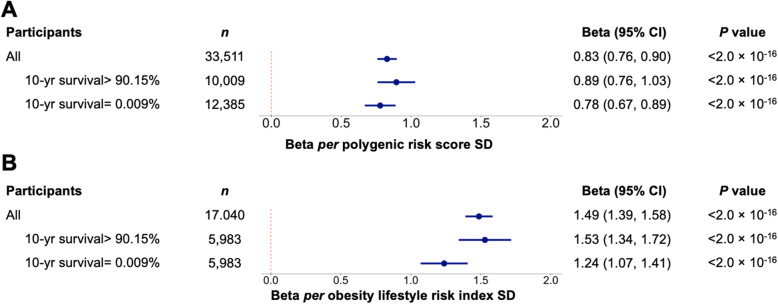
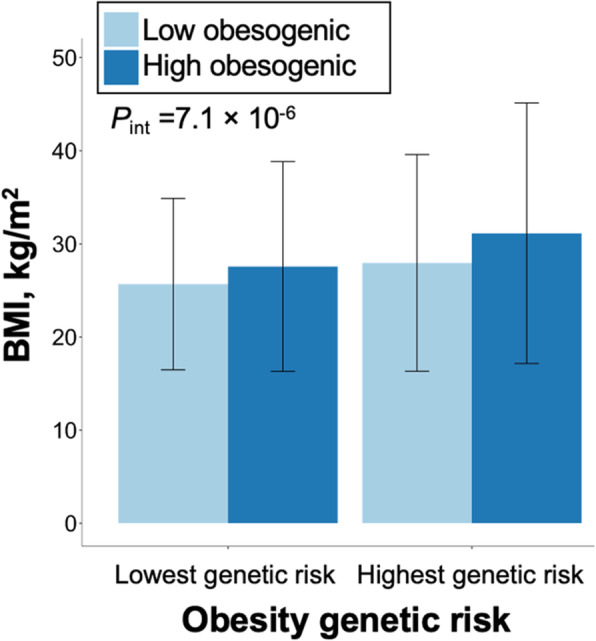
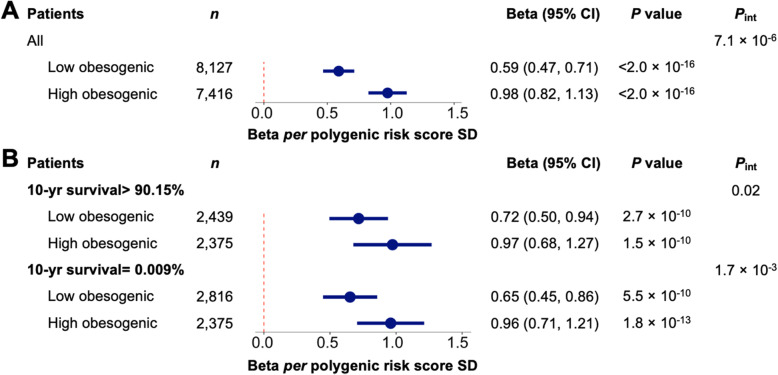
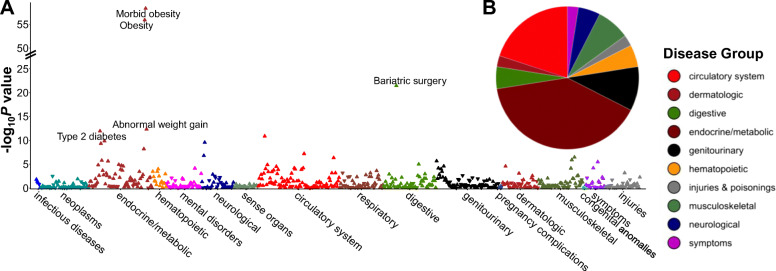
Thirty-three thousand five hundred eleven patients were analyzed (53.1% female; age 60.0 years; BMI 28.3 kg/m), of which 17,040 completed the lifestyle survey (57.5% female; age: 60.2; BMI: 28.1 (6.2) kg/m). Each standard deviation increment in the PRS was associated with 0.83 kg/m unit increase in BMI (95% confidence interval (CI) =0.76, 0.90). There was an interaction between the obesity PRS and obesity lifestyle risk index on BMI. The difference in BMI between those with a high and low obesogenic index was 3.18 kg/m in patients in the highest decile of PRS, whereas that difference was only 1.55 kg/m in patients in the lowest decile of PRS. In PheWAS, the obesity PRS was associated with 40 diseases spanning endocrine/metabolic, circulatory, and 8 other disease groups. No interactions were evident between the PRS and the index on disease outcomes.
In this hospital-based clinical biobank, obesity risk conferred by common genetic variants was associated with elevated BMI and this risk was attenuated by a healthier patient lifestyle. Continued consideration of the role of lifestyle in the context of genetic predisposition in healthcare settings is necessary to quantify the extent to which modifiable lifestyle risk factors may moderate genetic predisposition and inform clinical action to achieve personalized medicine.
遗传和生活方式因素对肥胖和相关疾病有很大影响,但它们在临床队列中的影响尚不清楚。本研究在一个患者生物库中,研究了体重指数多基因风险评分(PRS)及其与生活方式风险因素的相互作用与临床测量的体重指数和临床表型的关系。
马萨诸塞州综合医院生物库(MGB)是一个基于医院的队列,具有电子健康记录、遗传和生活方式数据。使用 97 个与 BMI 相关的遗传变异生成肥胖 PRS。肥胖生活方式风险指数是通过对肥胖生活方式风险因素(酒精、教育、运动、睡眠、吸烟和轮班工作)的调查反应来确定的,该指数将队列根据人群中位数分为高和低肥胖风险指数。在临床就诊时测量身高和体重。采用多变量线性横断面关联分析,分析 PRS 与 BMI 的关系,并分析与肥胖生活方式风险指数的相互作用。在表型全基因组关联分析(PheWAS)中,对来自计费代码的 675 种疾病结果进行了类似的逻辑模型分析。
分析了 33111 名患者(53.1%为女性;年龄 60.0 岁;BMI 28.3 kg/m),其中 17040 名完成了生活方式调查(57.5%为女性;年龄:60.2;BMI:28.1(6.2)kg/m)。PRS 每增加一个标准差,BMI 就会增加 0.83 kg/m(95%置信区间(CI)=0.76,0.90)。肥胖 PRS 与肥胖生活方式风险指数在 BMI 上存在交互作用。在 PRS 最高十分位数的患者中,高和低肥胖风险指数之间的 BMI 差异为 3.18 kg/m,而在 PRS 最低十分位数的患者中,这一差异仅为 1.55 kg/m。在 PheWAS 中,肥胖 PRS 与涵盖内分泌/代谢、循环和 8 个其他疾病组的 40 种疾病相关。PRS 与指数在疾病结果上没有明显的相互作用。
在这个基于医院的临床生物库中,常见遗传变异导致的肥胖风险与 BMI 升高有关,而这种风险会因患者生活方式更健康而减弱。在医疗保健环境中,需要继续考虑生活方式在遗传易感性背景下的作用,以量化可改变的生活方式风险因素可能减轻遗传易感性的程度,并为实现个性化医疗提供临床行动信息。