Kong Jian, Jiang Xiongying, Zhang Yanfang, Wang Weidong, Li Yong, Shen Xinying, Guo Jianxi, Sun Hongliang, Chen Dong, Chen Yaoting, Xu Linfeng
Department of Interventional Radiology, The First Affiliated Hospital of South University of Science and Technology, Second Clinical Medical College of Jinan University, Shenzhen People's Hospital, Shenzhen 518020, China.
Department of Interventional Radiology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou 510210, China.
Transl Cancer Res. 2020 Apr;9(4):2895-2903. doi: 10.21037/tcr.2020.03.65.
To summarize the incidence and management strategy of vascular lake (VL) during the treatment of hepatocellular carcinoma (HCC) using transarterial chemoembolization (TACE) with CalliSpheres drug-eluting beads (DEBs), and to analyze its relationship with tumor response rate (RR). The etiology and clinical significance of VL were also analyzed based on the available literature.
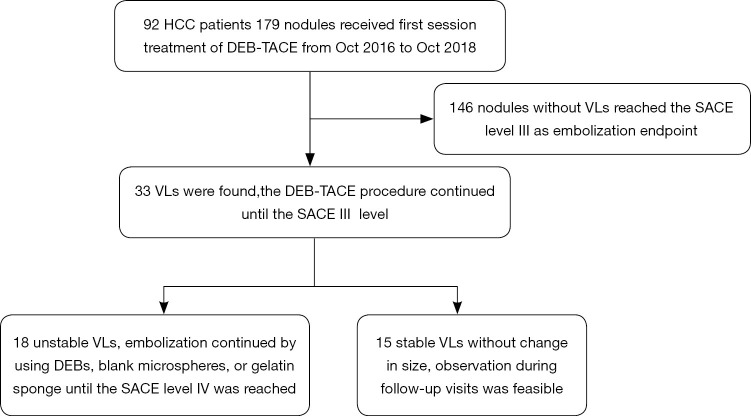
The clinical data of 92 HCC patients who were treated with chemoembolization using CalliSpheres DEBs (DEB-TACE) in two centers were retrospectively analyzed. All 92 patients were treatment-naïve and treated by DEB-TACE. The incidence of VL and its clinical treatment during the first embolization session were summarized. The lesions were divided into a VL group and a non-VL group to analyze the relationship between VL and tumor RR.
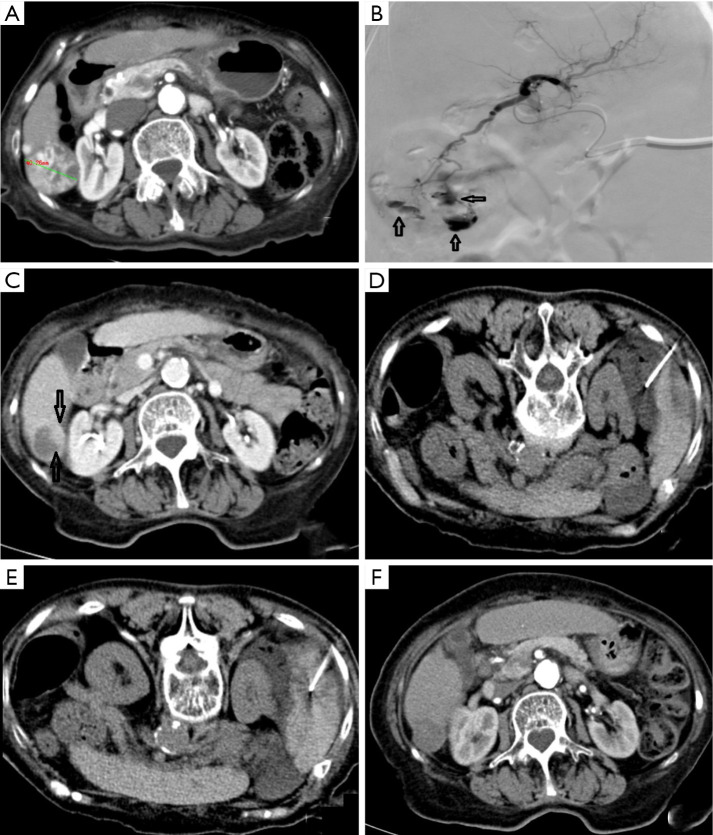
The embolization was successful in 98.9% of patients (91/92). A total of 33 VLs (18.4%; including 15 stable and 18 unstable VLs) were found among the 179 nodules treated. The unstable VLs were further embolized with embolic agent. One patient with unstable VL developed bleeding due to hepatic rupture and died. During the follow-up, residual tumors were found around 2 stable VLs, 2 lesions in 2 patients were treated with CT-guided radiofrequency ablation. The tumor RR was 84.4% in VL group, which was significantly higher than that (58.9%) in the non-VL group (P=0.007).
VL is a unique phenomenon during DEB-TACE. It may be accompanied by residual tumors and bleeding due to rupture. Therefore, VL should be cautiously managed in clinical practice.
总结使用载药微球(CalliSpheres)经动脉化疗栓塞术(TACE)治疗肝细胞癌(HCC)过程中血管湖(VL)的发生率及处理策略,并分析其与肿瘤反应率(RR)的关系。同时基于现有文献分析VL的病因及临床意义。
回顾性分析两个中心92例接受载药微球经动脉化疗栓塞术(DEB-TACE)治疗的HCC患者的临床资料。所有92例患者均为初治患者且接受DEB-TACE治疗。总结首次栓塞过程中VL的发生率及其临床处理情况。将病灶分为VL组和非VL组,分析VL与肿瘤RR的关系。
98.9%(91/92)的患者栓塞成功。在179个治疗结节中,共发现33个VL(18.4%;包括15个稳定型和18个不稳定型VL)。不稳定型VL用栓塞剂进一步栓塞。1例不稳定型VL患者因肝破裂出血死亡。随访期间,在2个稳定型VL周围发现残留肿瘤,2例患者的2个病灶接受了CT引导下射频消融治疗。VL组的肿瘤RR为84.4%,显著高于非VL组(58.9%)(P = 0.007)。
VL是DEB-TACE过程中的一种独特现象。它可能伴有残留肿瘤及破裂出血。因此,临床实践中应谨慎处理VL。