Theoretical and Applied Mechanics Program, McCormick School of Engineering, Northwestern University, Evanston, Illinois.
Department of Mechanical Engineering, McCormick School of Engineering, Northwestern University, Evanston, Illinois.
Am J Physiol Gastrointest Liver Physiol. 2022 May 1;322(5):G500-G512. doi: 10.1152/ajpgi.00281.2021. Epub 2022 Feb 16.
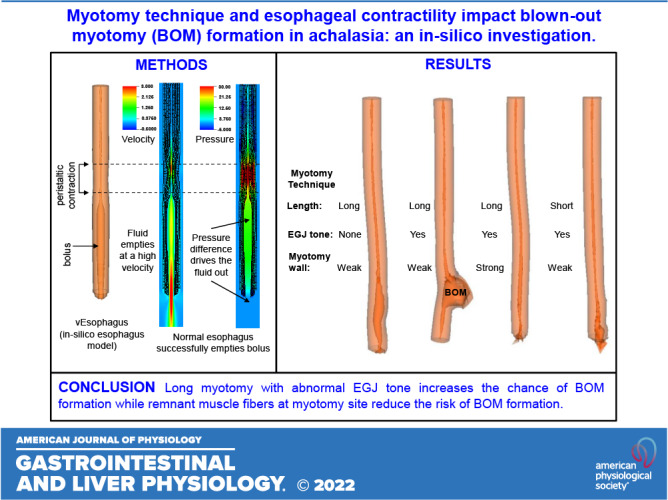
We used in silico models to investigate the impact of the dimensions of myotomy, contraction pattern, the tone of the esophagogastric junction (EGJ), and musculature at the myotomy site on esophageal wall stresses potentially leading to the formation of a blown-out myotomy (BOM). We performed three sets of simulations with an in silico esophagus model, wherein the myotomy-influenced region was modeled as an elliptical section devoid of muscle fibers. These sets investigated the effects of the dimensions of myotomy, differing esophageal contraction types, and differing esophagogastric junction (EGJ) tone and wall stiffness at the myotomy affected region on esophageal wall stresses potentially leading to BOM. Longer myotomy was found to be accompanied by a higher bolus volume accumulated at the myotomy site. With respect to esophageal contractions, deformation at the myotomy site was greatest with propagated peristalsis, followed by combined peristalsis and spasm, and pan-esophageal pressurization. Stronger EGJ tone with respect to the wall stiffness at the myotomy site was found to aid in increasing deformation at the myotomy site. In addition, we found that an esophagus with a shorter myotomy performed better at emptying the bolus than that with a longer myotomy. Shorter myotomies decrease the chance of BOM formation. Propagated peristalsis with EGJ outflow obstruction has the highest chance of BOM formation. We also found that abnormal residual EGJ tone may be a co-factor in the development of BOM, whereas remnant muscle fibers at myotomy site reduce the risk of BOM formation. Blown-out myotomy (BOM) is a complication observed after myotomy, which is performed to treat achalasia. In silico simulations were performed to identify the factors leading to BOM formation. We found that a short myotomy that is not transmural and has some structural architecture intact reduces the risk of BOM formation. In addition, we found that high esophagogastric junction tone due to fundoplication is found to increase the risk of BOM formation.
我们使用计算机模型来研究肌切开术的尺寸、收缩模式、食管胃结合部(EGJ)的紧张度以及肌切开部位的肌肉结构对食管壁张力的影响,这些张力可能导致切开术过度扩张(BOM)。我们使用计算机食管模型进行了三组模拟,其中肌切开术影响的区域被建模为没有肌纤维的椭圆形截面。这些模拟研究了肌切开术的尺寸、不同的食管收缩类型、不同的食管胃结合部(EGJ)紧张度和肌切开术影响区域的食管壁硬度对可能导致 BOM 的食管壁张力的影响。较长的肌切开术伴随着更多的食团在肌切开部位堆积。在食管收缩方面,在肌切开部位的变形以传播性蠕动最大,其次是蠕动和痉挛的组合,以及全食管加压。与肌切开术影响区域的壁硬度相比,EGJ 张力越强,在肌切开部位的变形越大。此外,我们发现排空食团的效果,短肌切开术优于长肌切开术。较短的肌切开术减少了 BOM 形成的机会。EGJ 流出阻塞时传播性蠕动有最高的 BOM 形成机会。我们还发现异常残留的 EGJ 张力可能是 BOM 发展的共同因素,而肌切开部位的残余肌肉纤维则降低了 BOM 形成的风险。切开术过度扩张(BOM)是肌切开术治疗贲门失弛缓症后的一种并发症。进行了计算机模拟以确定导致 BOM 形成的因素。我们发现,非穿透性且具有一些结构完整性的短肌切开术可降低 BOM 形成的风险。此外,我们发现由于胃底折叠术引起的高食管胃结合部张力会增加 BOM 形成的风险。