Department of Medicine and Surgery, University of Milan-Bicocca, Monza, Italy.
Department of Anesthesia and Intensive Care Medicine, Niguarda Ca' Granda, Milan, Italy.
Neurocrit Care. 2022 Aug;37(1):102-110. doi: 10.1007/s12028-022-01450-1. Epub 2022 Feb 23.
Hyperventilation resulting in hypocapnic alkalosis (HA) is frequently encountered in spontaneously breathing patients with acute cerebrovascular conditions. The underlying mechanisms of this respiratory response have not been fully elucidated. The present study describes, applying the physical-chemical approach, the acid-base characteristics of cerebrospinal fluid (CSF) and arterial plasma of spontaneously breathing patients with aneurismal subarachnoid hemorrhage (SAH) and compares these results with those of control patients. Moreover, it investigates the pathophysiologic mechanisms leading to HA in SAH.
Patients with SAH admitted to the neurological intensive care unit and patients (American Society of Anesthesiologists physical status of 1 and 2) undergoing elective surgery under spinal anesthesia were enrolled. CSF and arterial samples were collected simultaneously. Electrolytes, strong ion difference (SID), partial pressure of carbon dioxide (PCO), weak noncarbonic acids (A), and pH were measured in CSF and arterial blood samples.
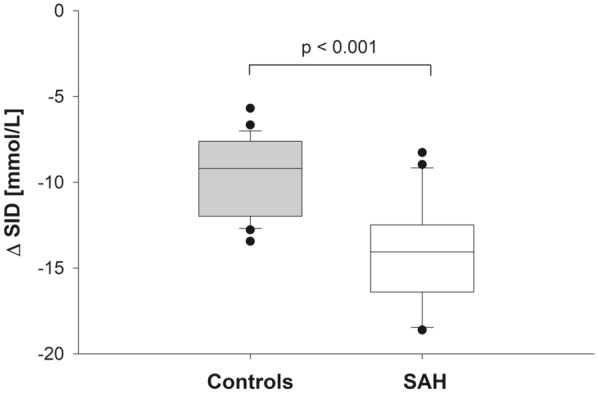
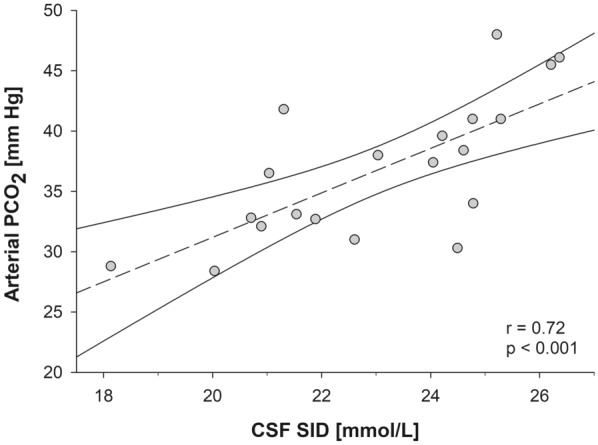
Twenty spontaneously breathing patients with SAH and 25 controls were enrolled. The CSF of patients with SAH, as compared with controls, was characterized by a lower SID (23.1 ± 2.3 vs. 26.5 ± 1.4 mmol/L, p < 0.001) and PCO (40 ± 4 vs. 46 ± 3 mm Hg, p < 0.001), whereas no differences in A (1.2 ± 0.5 vs. 1.2 ± 0.2 mmol/L, p = 0.95) and pH (7.34 ± 0.06 vs. 7.35 ± 0.02, p = 0.69) were observed. The reduced CSF SID was mainly caused by a higher lactate concentration (3.3 ± 1.3 vs. 1.4 ± 0.2 mmol/L, p < 0.001). A linear association (r = 0.71, p < 0.001) was found between CSF SID and arterial PCO. A higher proportion of patients with SAH were characterized by arterial HA, as compared with controls (40 vs. 4%, p = 0.003). A reduced CSF-to-plasma difference in PCO was observed in nonhyperventilating patients with SAH (0.4 ± 3.8 vs. 7.8 ± 3.7 mm Hg, p < 0.001).
Patients with SAH have a reduction of CSF SID due to an increased lactate concentration. The resulting localized acidifying effect is compensated by CSF hypocapnia, yielding normal CSF pH values and resulting in a higher incidence of arterial HA.
在患有急性脑血管疾病的自主呼吸患者中,常出现过度通气导致的低碳酸血症性碱中毒(HA)。这种呼吸反应的潜在机制尚未完全阐明。本研究应用物理化学方法描述了蛛网膜下腔出血(SAH)自主呼吸患者脑脊液(CSF)和动脉血浆的酸碱特征,并将这些结果与对照组进行比较。此外,还研究了导致 SAH 发生 HA 的病理生理机制。
纳入了入住神经重症监护病房的 SAH 患者和接受脊髓麻醉下择期手术的美国麻醉医师协会身体状况为 1 级和 2 级的患者。同时采集 CSF 和动脉样本。测量 CSF 和动脉血样本中的电解质、强离子差(SID)、二氧化碳分压(PCO)、弱非碳酸酸(A)和 pH。
共纳入 20 例 SAH 自主呼吸患者和 25 例对照组。与对照组相比,SAH 患者的 CSF 具有更低的 SID(23.1±2.3 对 26.5±1.4 mmol/L,p<0.001)和 PCO(40±4 对 46±3 mm Hg,p<0.001),而 A(1.2±0.5 对 1.2±0.2 mmol/L,p=0.95)和 pH(7.34±0.06 对 7.35±0.02,p=0.69)无差异。较低的 CSF SID 主要是由于乳酸浓度升高(3.3±1.3 对 1.4±0.2 mmol/L,p<0.001)。CSF SID 与动脉 PCO 之间存在线性关联(r=0.71,p<0.001)。与对照组相比,更多的 SAH 患者表现为动脉性 HA(40%对 4%,p=0.003)。在非过度通气的 SAH 患者中,CSF 与血浆 PCO 的差值减小(0.4±3.8 对 7.8±3.7 mm Hg,p<0.001)。
SAH 患者由于乳酸浓度升高而导致 CSF SID 降低。由此产生的局部酸化作用被 CSF 低碳酸血症所代偿,导致正常 CSF pH 值,并导致更高的动脉性 HA 发生率。