Pritchard Daryl, Patel Jai N, Stephens Lindsay E, McLeod Howard L
Personalized Medicine Coalition, Washington, DC, USA.
Department of Cancer Pharmacology and Pharmacogenomics, Levine Cancer Institute, Atrium Health, Charlotte, NC, USA.
Am J Health Syst Pharm. 2022 Jun 7;79(12):993-1005. doi: 10.1093/ajhp/zxac064.
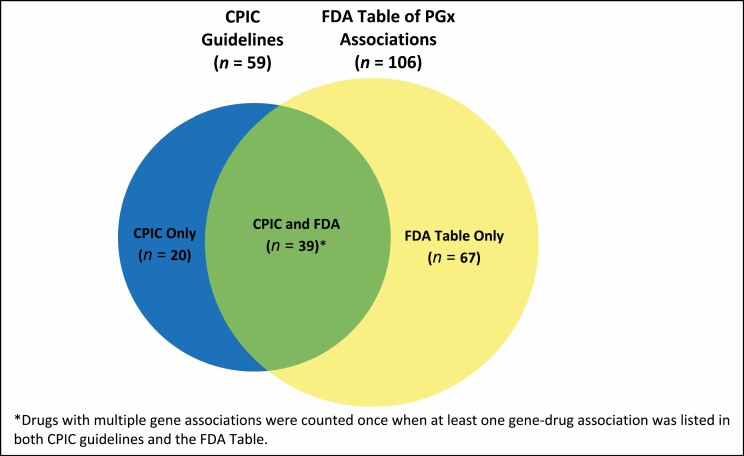
Healthcare professionals need a clear understanding of information about gene-drug interactions in order to make optimal use of pharmacogenetic (PGx) testing. In this report, we compare PGx information in the US Food and Drug Administration (FDA) Table of Pharmacogenetic Associations with information presented in Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines.
Information from CPIC guidelines and the FDA Table of Pharmacogenetic Associations do not have a high level of concordance. Many drugs mentioned in CPIC guidelines are not listed in the FDA table and vice versa, and the same gene-drug association and dosing recommendation was reported for only 5 of the 126 drugs included in either source. Furthermore, classification of drugs in specific sections of the FDA table does not correlate well with CPIC-assigned or provisionally assigned clinical actionability levels. The Pharmacogenomics Knowledge Base (PharmGKB) clinical annotation levels are generally high for drugs mentioned in CPIC guidelines. PharmGKB clinical annotation levels are often unassigned or are lower level for drugs listed on the FDA table but not in CPIC guidelines. These differences may be due in part to FDA having access to PGx information that is unavailable in published literature and/or because PGx classifications are based on criteria other than clinical actionability.
There are important differences between the PGx information presented in the FDA Table of Pharmacogenetic Associations and in CPIC guidelines. FDA and CPIC have different perspectives when evaluating PGx associations and use different approaches and information resources when considering clinical validity related to specific medicines. Understanding how information sources developed by each group differ and can be used together to form a holistic view of PGx may be helpful in increasing adoption of these information sources in practice.
医疗保健专业人员需要清楚地了解基因-药物相互作用的信息,以便最佳地利用药物基因组学(PGx)检测。在本报告中,我们比较了美国食品药品监督管理局(FDA)药物基因组学关联表中的PGx信息与临床药物基因组学实施联盟(CPIC)指南中提供的信息。
CPIC指南和FDA药物基因组学关联表中的信息一致性不高。CPIC指南中提到的许多药物未列入FDA表中,反之亦然,并且在这两个来源所包含的126种药物中,只有5种报告了相同的基因-药物关联和给药建议。此外,FDA表中特定部分的药物分类与CPIC指定或临时指定的临床可操作性水平相关性不佳。CPIC指南中提到的药物,药物基因组学知识库(PharmGKB)的临床注释水平通常较高。对于FDA表中列出但不在CPIC指南中的药物,PharmGKB临床注释水平通常未指定或较低。这些差异可能部分是由于FDA能够获取已发表文献中没有的PGx信息,和/或因为PGx分类基于临床可操作性以外的标准。
FDA药物基因组学关联表和CPIC指南中呈现的PGx信息存在重要差异。FDA和CPIC在评估PGx关联时观点不同,在考虑与特定药物相关的临床有效性时使用不同的方法和信息资源。了解每个组织开发的信息来源如何不同以及如何一起使用以形成PGx的整体视图,可能有助于在实践中更多地采用这些信息来源。