Department of Medicine A,Hematology,Oncology and Pulmonary Medicine, University Hospital Münster, Münster, Germany.
Department of Medicine B for Gastroenterology,Hepatology,Endocrinology and Clinical Infectiology, University Hospital Münster, Münster, Germany.
Can Respir J. 2022 Mar 1;2022:2466789. doi: 10.1155/2022/2466789. eCollection 2022.
Following COVID-19, patients often present with ongoing symptoms comparable to chronic fatigue and subjective deterioration of exercise capacity (EC), which has been recently described as postacute COVID-19 syndrome.
To objectify the reduced EC after COVID-19 and to evaluate for pathologic limitations.
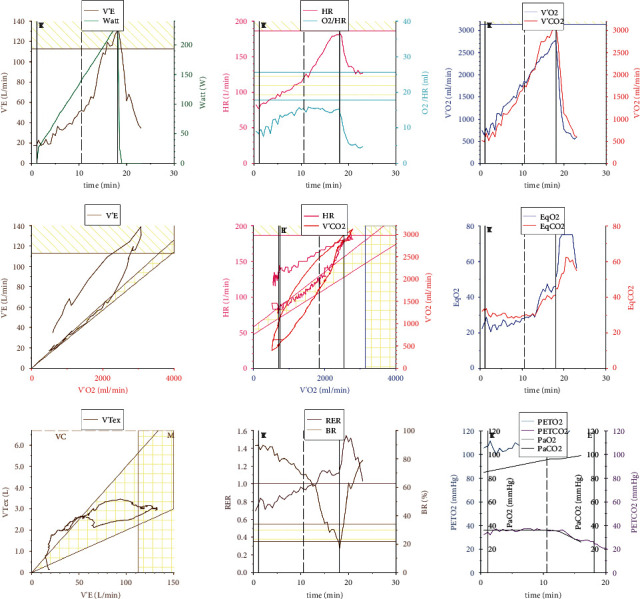
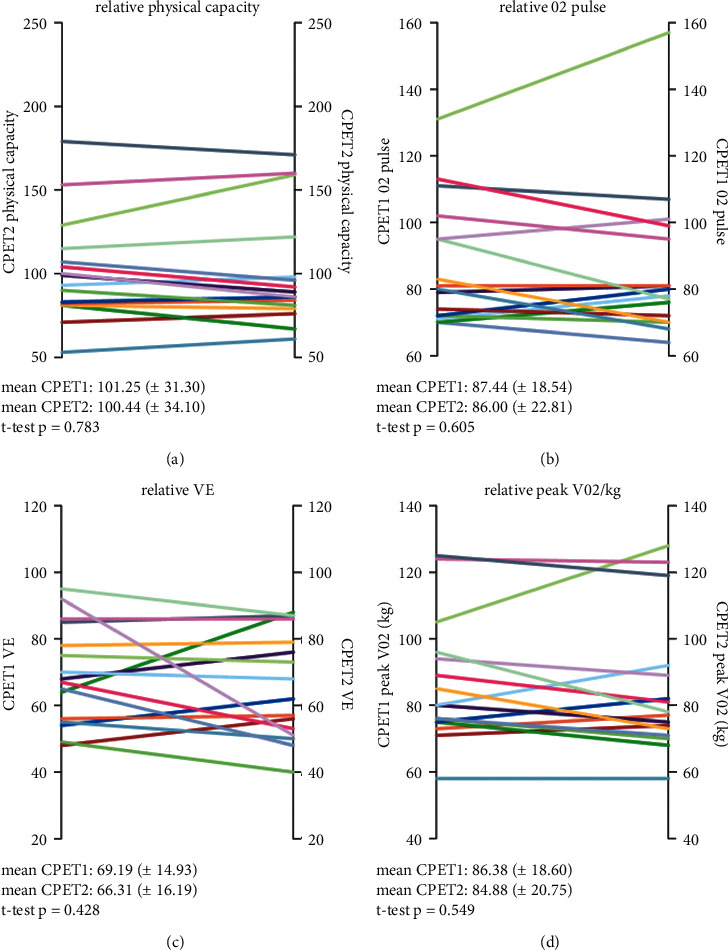
Thirty patients with subjective limitation of EC performed cardiopulmonary exercise testing (CPET). If objectively limited in EC or deteriorated in oxygen pulse, we offered cardiac stress magnetic resonance imaging (MRI) and a follow-up CPET.
Eighteen male and 12 female patients were included. Limited relative EC was detected in 11/30 (36.7%) patients. Limitation correlated with reduced body weight-indexed peak oxygen (O) uptake (peakV̇O/kg) (mean 74.7 (±7.1) % vs. 103.6 (±14.9) %, < 0.001). Reduced peakV̇O/kg was found in 18/30 (60.0%) patients with limited EC. Patients with reduced EC widely presented an impaired maximum O pulse (75.7% (±5.6) vs. 106.8% (±13.9), < 0.001). Abnormal gas exchange was absent in all limited EC patients. Moreover, no patient showed signs of reduced pulmonary perfusion. Using cardiac MRI, diminished biventricular ejection fraction was ruled out in 16 patients as a possible cause for reduced O pulse. Despite noncontrolled training exercises, follow-up CPET did not reveal any exercise improvements.
Deterioration of EC was not associated with ventilatory or pulmonary vascular limitation. Exercise limitation was related to both reduced O pulse and peakV̇O/kg, which, however, did not correlate with the initial severity of COVID-19. We hypothesize that impaired microcirculation or limited peripheral O utilization might be causative for prolonged deterioration of EC following acute COVID-19 infection.
新冠病毒感染后,患者常出现类似于慢性疲劳的持续症状,并伴有运动能力(EC)的主观恶化,这种情况最近被描述为新冠后急性综合征。
客观评估新冠后运动能力的降低,并评估其是否存在病理性限制。
30 名主观运动能力受限的患者进行心肺运动测试(CPET)。如果 EC 受限或氧脉搏恶化,则进行心脏应激磁共振成像(MRI)检查和后续 CPET。
纳入 18 名男性和 12 名女性患者。30 名患者中,11 名(36.7%)存在相对受限的 EC。限制与体重指数校正峰值摄氧量(peakV̇O/kg)降低相关(平均 74.7(±7.1)%比 103.6(±14.9)%,<0.001)。30 名患者中,18 名(60.0%)存在受限的 peakV̇O/kg。表现为运动能力受限的患者,其最大氧脉搏明显降低(75.7%(±5.6)比 106.8%(±13.9)%,<0.001)。所有受限 EC 患者的气体交换均未见异常。此外,没有患者显示肺灌注减少的迹象。使用心脏 MRI,16 名患者排除了双心室射血分数降低作为降低氧脉搏的可能原因。尽管进行了非控制的训练运动,但后续 CPET 并未显示任何运动能力的改善。
EC 恶化与通气或肺血管限制无关。运动受限与氧脉搏和 peakV̇O/kg 降低有关,但与新冠病毒感染的初始严重程度无关。我们假设,急性新冠病毒感染后,微循环受损或外周氧利用受限可能是运动能力持续恶化的原因。