Liu Gui, Mugo Nelly R, Bayer Cara, Rao Darcy White, Onono Maricianah, Mgodi Nyaradzo M, Chirenje Zvavahera M, Njoroge Betty W, Tan Nicholas, Bukusi Elizabeth A, Barnabas Ruanne V
Department of Global Health, University of Washington, Seattle, USA.
Kenya Medical Research Institute, Nairobi, Kenya.
EClinicalMedicine. 2022 Feb 19;45:101306. doi: 10.1016/j.eclinm.2022.101306. eCollection 2022 Mar.
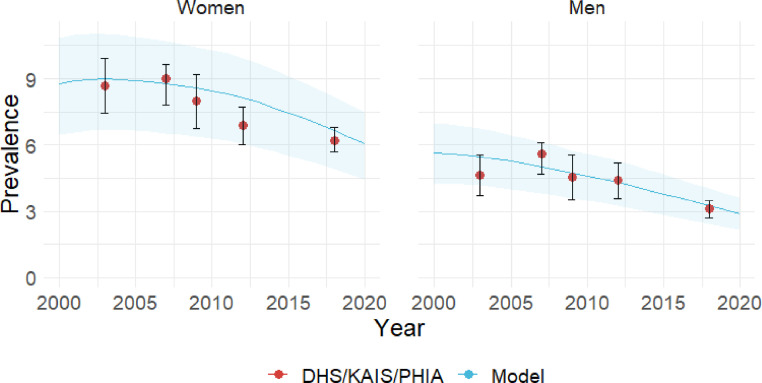
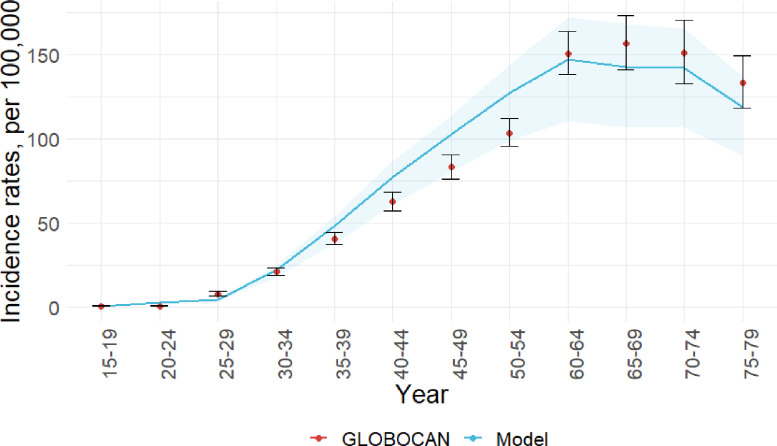
Cervical cancer incidence is high in Kenya due to HIV and limited access to cancer prevention services. Human papillomavirus (HPV) has been shown to increase HIV acquisition; however, the potential impact of HPV vaccination on HIV is unknown. We modeled the health impact of HPV vaccination in the context of the HIV epidemiology in Kenya.
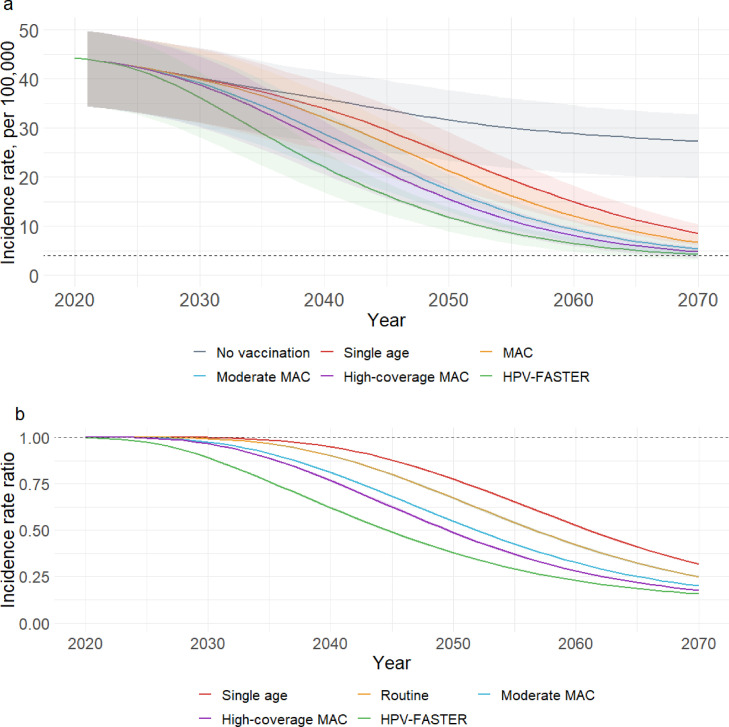
Using a validated compartmental transmission model of HIV and HPV set in Kenya, we evaluated five scenarios of nonavalent HPV vaccination: single-age-vaccination of 10-year-old girls at 90% coverage; multi-age-cohort (MAC) vaccination of 10-14-year-old girls at 90% coverage; MAC plus moderate-coverage (50%) catch-up vaccination of 15-24-year-old women; MAC plus high-coverage (80%) catch-up of 15-24-year-old women; and MAC plus catch-up of 15-44-year-old women at 80% coverage (HPV-FASTER). We compared cervical cancer incidence, HIV prevalence, and cumulative cervical cancer and HIV cases averted after 50 years to a baseline scenario without vaccination. In all scenarios, we assumed the UNAIDS 90-90-90 goal for HIV treatment is attained by 2030.
In 2021, model-estimated cervical cancer incidence is 44/100,000 and HIV prevalence among women is 6·5%. In 2070, projected cancer incidence declines to 27/100,000 and HIV prevalence reaches 0·3% without vaccination. With single-age-vaccination, cancer incidence in 2070 is reduced by 68%, averting 64,529 cumulative cancer cases. MAC vaccination reduces cancer incidence by 75%, averting 206,115 cancer cases. Moderate and high-coverage catch-up and HPV-FASTER reduce cancer incidence by 80%, 82%, and 84%, averting 254,930, 278,690, and 326,968 cancer cases, respectively. In all scenarios, HIV prevalence in 2070 is reduced by a relative 8-11%, with 15,609-34,981 HIV cases averted after 50 years.
HPV vaccination can substantially reduce cervical cancer incidence in Kenya in the next 50 years, particularly if women up to age 24 are vaccinated. HIV treatment scale-up can also alleviate cervical cancer burden. However, HPV vaccination has modest additional impact on HIV when antiretroviral therapy coverage is high.
National Institutes of Health, Bill and Melinda Gates Foundation.
由于艾滋病毒感染率高且获得癌症预防服务的机会有限,肯尼亚宫颈癌发病率很高。人乳头瘤病毒(HPV)已被证明会增加艾滋病毒感染风险;然而,HPV疫苗接种对艾滋病毒的潜在影响尚不清楚。我们在肯尼亚艾滋病毒流行病学背景下对HPV疫苗接种的健康影响进行了建模。
使用在肯尼亚建立的经过验证的艾滋病毒和HPV的分区传播模型,我们评估了九价HPV疫苗接种的五种方案:对10岁女孩进行单一年龄组接种,接种覆盖率为90%;对10至14岁女孩进行多年龄队列(MAC)接种,接种覆盖率为90%;MAC接种加上对15至24岁女性进行中等覆盖率(50%)的补种;MAC接种加上对15至24岁女性进行高覆盖率(80%)的补种;以及MAC接种加上对15至44岁女性进行80%覆盖率的补种(HPV-FASTER)。我们将50年后宫颈癌发病率、艾滋病毒流行率以及避免的宫颈癌和艾滋病毒累积病例数与未接种疫苗的基线情况进行了比较。在所有方案中,我们假设到2030年实现联合国艾滋病规划署的艾滋病毒治疗90-90-90目标。
2021年,模型估计的宫颈癌发病率为44/10万,女性中的艾滋病毒流行率为6.5%。到2070年,预计在未接种疫苗的情况下,癌症发病率将降至27/10万,艾滋病毒流行率将达到0.3%。进行单一年龄组接种后,2070年的癌症发病率降低了68%,避免了64529例累积癌症病例。MAC接种使癌症发病率降低了75%,避免了206115例癌症病例。中等覆盖率和高覆盖率的补种以及HPV-FASTER分别使癌症发病率降低了80%、82%和84%,避免了254930例、278690例和326968例癌症病例。在所有方案中,2070年的艾滋病毒流行率相对降低了8%-11%,50年后避免了15609-34981例艾滋病毒病例。
HPV疫苗接种可在未来50年内大幅降低肯尼亚的宫颈癌发病率,特别是如果对24岁及以下的女性进行接种。扩大艾滋病毒治疗规模也可减轻宫颈癌负担。然而,当抗逆转录病毒疗法覆盖率较高时,HPV疫苗接种对艾滋病毒的额外影响较小。
美国国立卫生研究院、比尔及梅琳达·盖茨基金会。