Bidar Frank, Hamada Sarah, Gossez Morgane, Coudereau Remy, Lopez Jonathan, Cazalis Marie-Angelique, Tardiveau Claire, Brengel-Pesce Karen, Mommert Marine, Buisson Marielle, Conti Filippo, Rimmelé Thomas, Lukaszewicz Anne-Claire, Argaud Laurent, Cour Martin, Monneret Guillaume, Venet Fabienne
Joint Research Unit HCL-bioMérieux, EA 7426 "Pathophysiology of Injury-Induced Immunosuppression", Université Claude Bernard Lyon, 1-Hospices Civils de Lyon-bioMérieux, 69003, Lyon, France.
Anesthesia and Critical Care Medicine Department, Edouard Herriot Hospital, Hospices Civils de Lyon, 69437, Lyon, France.
Ann Intensive Care. 2022 Mar 5;12(1):21. doi: 10.1186/s13613-022-00982-1.
Lymphopenia is a hallmark of severe coronavirus disease 19 (COVID-19). Similar alterations have been described in bacterial sepsis and therapeutic strategies targeting T cell function such as recombinant human interleukin 7 (rhIL-7) have been proposed in this clinical context. As COVID-19 is a viral sepsis, the objectives of this study were to characterize T lymphocyte response over time in severe COVID-19 patients and to assess the effect of ex vivo administration of rhIL-7.
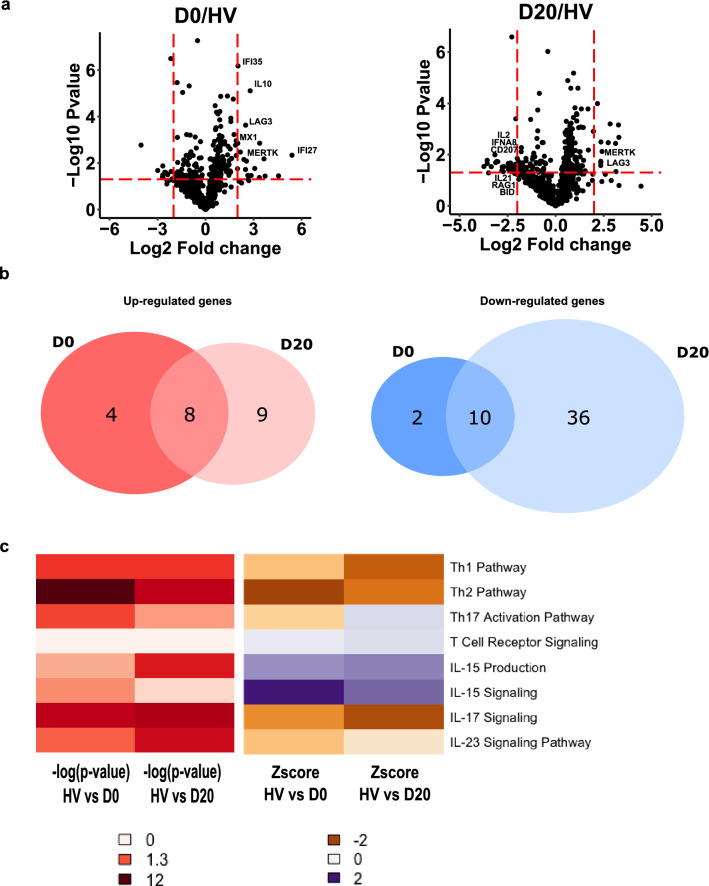
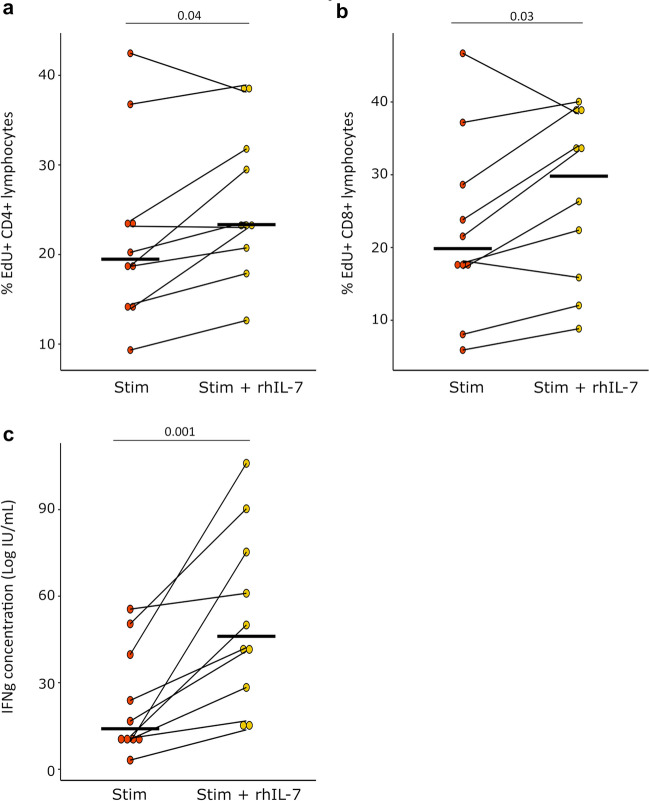
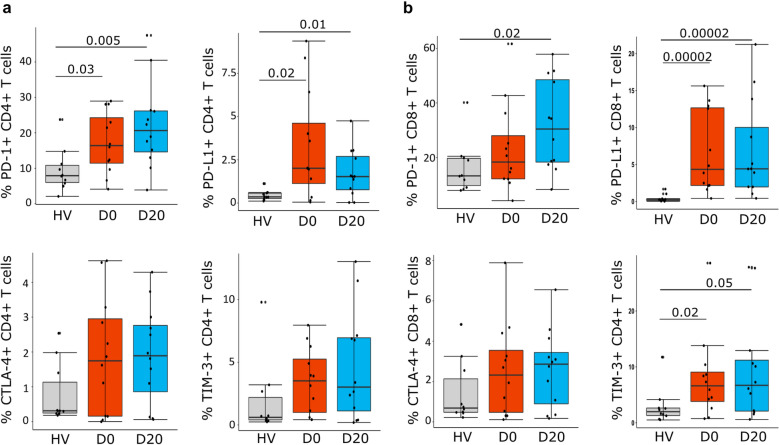
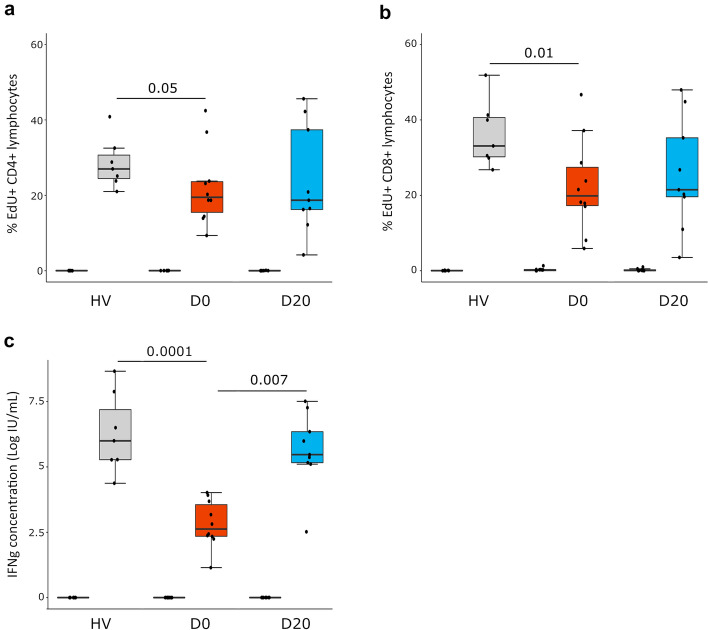
Peripheral blood mononuclear cells from COVID-19 patients hospitalized in intensive care unit (ICU) were collected at admission and after 20 days. Transcriptomic profile was evaluated through NanoString technology. Inhibitory immune checkpoints expressions were determined by flow cytometry. T lymphocyte proliferation and IFN-γ production were evaluated after ex vivo stimulation in the presence or not of rhIL-7. COVID-19 ICU patients were markedly lymphopenic at admission. Mononuclear cells presented with inhibited transcriptomic profile prevalently with impaired T cell activation pathways. CD4 + and CD8 + T cells presented with over-expression of co-inhibitory molecules PD-1, PD-L1, CTLA-4 and TIM-3. CD4 + and CD8 + T cell proliferation and IFN-γ production were markedly altered in samples collected at ICU admission. These alterations, characteristic of a T cell exhaustion state, were more pronounced at ICU admission and alleviated over time. Treatment with rhIL-7 ex vivo significantly improved both T cell proliferation and IFN-γ production in cells from COVID-19 patients.
Severe COVID-19 patients present with features of profound T cell exhaustion upon ICU admission which can be reversed ex vivo by rhIL-7. These results reinforce our understanding of severe COVID-19 pathophysiology and opens novel therapeutic avenues to treat such critically ill patients based of immunomodulation approaches. Defining the appropriate timing for initiating such immune-adjuvant therapy in clinical setting and the pertinent markers for a careful selection of patients are now warranted to confirm the ex vivo results described so far. Trial registration ClinicalTrials.gov identifier: NCT04392401 Registered 18 May 2020, http:// clinicaltrials.gov/ct2/show/NCT04392401.
淋巴细胞减少是重症冠状病毒病19(COVID-19)的一个标志。在细菌性脓毒症中也描述了类似的改变,并且在这种临床背景下已经提出了针对T细胞功能的治疗策略,例如重组人白细胞介素7(rhIL-7)。由于COVID-19是一种病毒性脓毒症,本研究的目的是描述重症COVID-19患者T淋巴细胞反应随时间的变化,并评估rhIL-7体外给药的效果。
在重症监护病房(ICU)住院的COVID-19患者入院时和20天后采集外周血单个核细胞。通过NanoString技术评估转录组谱。通过流式细胞术测定抑制性免疫检查点的表达。在有或没有rhIL-7的情况下,体外刺激后评估T淋巴细胞增殖和IFN-γ产生。COVID-19 ICU患者入院时明显淋巴细胞减少。单个核细胞呈现转录组谱受抑制,主要是T细胞活化途径受损。CD4 +和CD8 + T细胞呈现共抑制分子PD-1、PD-L1、CTLA-4和TIM-3的过表达。在ICU入院时采集的样本中,CD4 +和CD8 + T细胞增殖以及IFN-γ产生明显改变。这些T细胞耗竭状态的特征在ICU入院时更明显,并随时间缓解。rhIL-7体外治疗显著改善了COVID-19患者细胞中的T细胞增殖和IFN-γ产生。
重症COVID-19患者在ICU入院时呈现出深度T细胞耗竭的特征,这可以通过rhIL-7在体外逆转。这些结果加强了我们对重症COVID-19病理生理学的理解,并为基于免疫调节方法治疗此类重症患者开辟了新的治疗途径。现在有必要确定在临床环境中启动这种免疫辅助治疗的合适时机以及用于仔细选择患者的相关标志物,以确认迄今为止所描述的体外结果。试验注册ClinicalTrials.gov标识符:NCT04392401,于2020年5月18日注册,http://clinicaltrials.gov/ct2/show/NCT04392401 。