Department of Urology, Freeman Hospital, Newcastle upon Tyne, UK.
Translational and Clinical Research Institute, William Leech Building, The Medical School, Newcastle upon Tyne, UK.
BMJ. 2022 Mar 9;376:e068229. doi: 10.1136/bmj-2021-0068229.
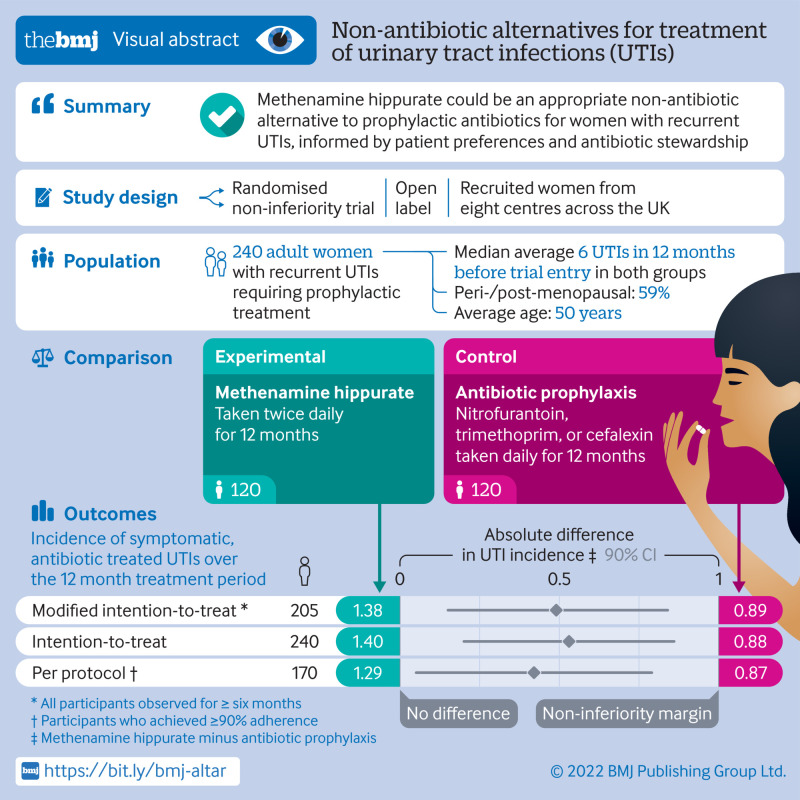
To test and compare the efficacy of methenamine hippurate for prevention of recurrent urinary tract infections with the current standard prophylaxis of daily low dose antibiotics.
Multicentre, open label, randomised, non-inferiority trial.
Eight centres in the UK, recruiting from June 2016 to June 2018.
Women aged ≥18 years with recurrent urinary tract infections, requiring prophylactic treatment.
Random assignment (1:1, using permuted blocks of variable length via a web based system) to receive antibiotic prophylaxis or methenamine hippurate for 12 months. Treatment allocation was not masked and crossover between arms was allowed.
Absolute difference in incidence of symptomatic, antibiotic treated, urinary tract infections during treatment. A patient and public involvement group predefined the non-inferiority margin as one episode of urinary tract infection per person year. Analyses performed in a modified intention-to-treat population comprised all participants observed for at least six months.
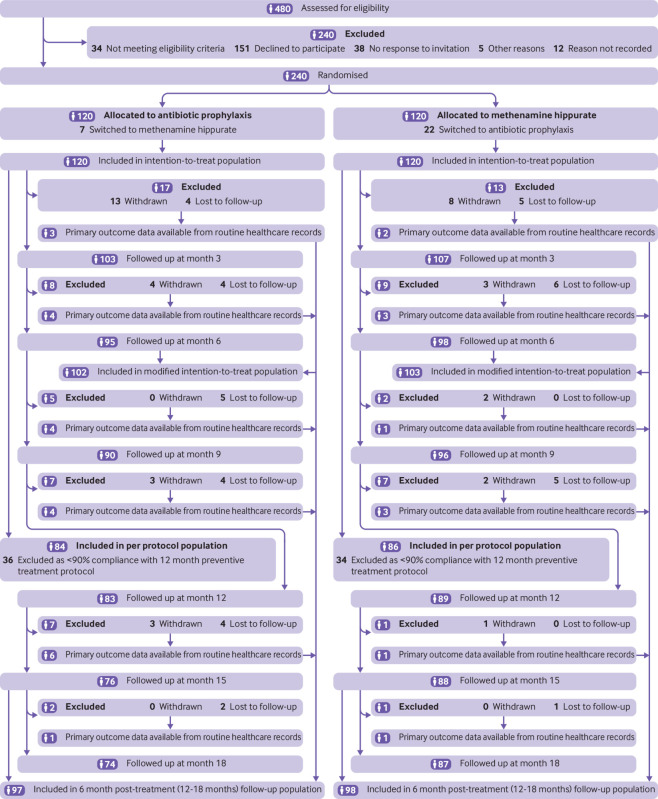
Participants were randomly assigned to antibiotic prophylaxis (n=120) or methenamine hippurate (n=120). The modified intention-to-treat analysis comprised 205 (85%) participants (antibiotics, n=102 (85%); methenamine hippurate, n=103 (86%)). Incidence of antibiotic treated urinary tract infections during the 12 month treatment period was 0.89 episodes per person year (95% confidence interval 0.65 to 1.12) in the antibiotics group and 1.38 (1.05 to 1.72) in the methenamine hippurate group, with an absolute difference of 0.49 (90% confidence interval 0.15 to 0.84) confirming non-inferiority. Adverse reactions were reported by 34/142 (24%) in the antibiotic group and 35/127 (28%) in the methenamine group and most reactions were mild.
Non-antibiotic prophylactic treatment with methenamine hippurate might be appropriate for women with a history of recurrent episodes of urinary tract infections, informed by patient preferences and antibiotic stewardship initiatives, given the demonstration of non-inferiority to daily antibiotic prophylaxis seen in this trial.
ISRCTN70219762.
测试并比较三聚氰胺尿酸盐预防复发性尿路感染的疗效与目前每日低剂量抗生素标准预防的疗效。
多中心、开放标签、随机、非劣效性试验。
英国 8 个中心,于 2016 年 6 月至 2018 年 6 月招募参与者。
年龄≥18 岁的复发性尿路感染女性,需要预防治疗。
随机分配(1:1,通过基于网络的系统使用可变长度的置换块)接受抗生素预防或三聚氰胺尿酸盐治疗 12 个月。治疗分配未设盲,允许臂间交叉。
治疗期间症状性、抗生素治疗的尿路感染的绝对发生率差异。一个患者和公众参与小组将非劣效性边界定义为每人每年发生一次尿路感染。在至少观察 6 个月的所有参与者的修改后的意向治疗人群中进行分析。
参与者被随机分配至抗生素预防组(n=120)或三聚氰胺尿酸盐组(n=120)。修改后的意向治疗分析包括 205 名(85%)参与者(抗生素组,n=102(85%);三聚氰胺尿酸盐组,n=103(86%))。在 12 个月的治疗期间,抗生素组发生抗生素治疗的尿路感染的发生率为 0.89 例/人年(95%置信区间 0.65 至 1.12),三聚氰胺尿酸盐组为 1.38(1.05 至 1.72),绝对差异为 0.49(90%置信区间 0.15 至 0.84),证实了非劣效性。抗生素组有 34/142(24%)和三聚氰胺尿酸盐组有 35/127(28%)报告了不良反应,大多数反应为轻度。
鉴于本试验显示非抗生素预防性三聚氰胺尿酸盐治疗与每日抗生素预防相比不劣效,对于有反复发作尿路感染病史的女性,根据患者的偏好和抗生素管理计划,这种治疗可能是合适的。
ISRCTN70219762。