Zhang Anbing, Xia Xiuqiong, Yuan Xiaoling, Liu Yuxia, Niu Haiming, Zhang Yinying, Liang Jianping
Department of Respiratory and Critical Care Medicine, Zhongshan People's Hospital, Zhongshan, People's Republic of China.
Department of Intensive Care Unit, Zhongshan People's Hospital, Zhongshan, People's Republic of China.
Infect Drug Resist. 2022 Mar 6;15:873-881. doi: 10.2147/IDR.S355024. eCollection 2022.
To explore the clinical characteristics, diagnosis, and treatment of severe pneumonia complicated by rhabdomyolysis and to improve the success rate of treatment.
The clinical characteristics, diagnosis, treatment, and outcomes of four patients with severe pneumonia complicated by rhabdomyolysis diagnosed by metagenomic next-generation sequencing (mNGS) in our hospital were analyzed retrospectively.
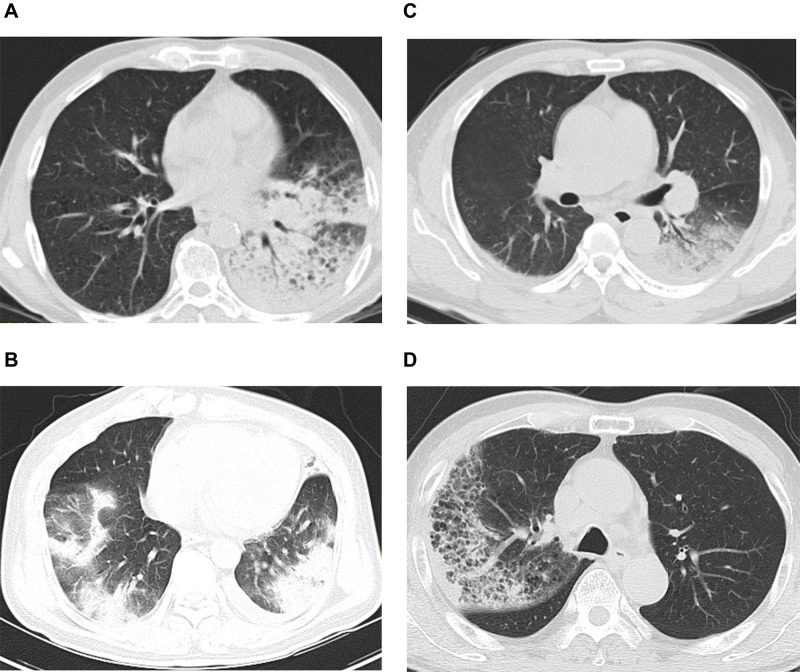
All four patients were male, aged 46-64 years, and all had a history of bird contact. All patients had fever, fatigue, tea-colored urine, myalgia, and two patients were unable to walk. DNA was found by mNGS of the bronchoalveolar lavage fluid of all four patients. Their creatine kinase was >1000 U/L, and myoglobin, C-reactive protein, procalcitonin, and brain natriuretic peptide were significantly increased. The McMahon score of three patients was >6 points, of whom one patient suffered from acute kidney injury; he was treated with continuous renal replacement therapy and eventually died. After diagnosis, three patients were treated with doxycycline and quinolones and were discharged after recovery.
Psittacosis complicated by rhabdomyolysis is characterized by fever, fatigue, myalgia, and tea-colored urine, with significant increases in creatine kinase and myoglobin. The McMahon score should be applied early to assess the risk of acute kidney injury, and renal replacement therapy and renal protection therapy should be initiated in the early stage. Among severely ill patients, early use of empirical antibiotics, including quinolones, may improve the prognosis.
探讨重症肺炎合并横纹肌溶解的临床特征、诊断及治疗方法,以提高治疗成功率。
回顾性分析我院4例经宏基因组下一代测序(mNGS)诊断为重症肺炎合并横纹肌溶解患者的临床特征、诊断、治疗及转归。
4例患者均为男性,年龄46 - 64岁,均有鸟类接触史。所有患者均有发热、乏力、茶色尿、肌痛,2例患者无法行走。4例患者支气管肺泡灌洗液mNGS均发现病原体DNA。其肌酸激酶>1000 U/L,肌红蛋白、C反应蛋白、降钙素原及脑钠肽均显著升高。3例患者麦克马洪评分>6分,其中1例发生急性肾损伤;经持续肾脏替代治疗,最终死亡。确诊后,3例患者应用多西环素及喹诺酮类药物治疗,康复后出院。
鹦鹉热合并横纹肌溶解症以发热、乏力、肌痛及茶色尿为特征,肌酸激酶及肌红蛋白显著升高。应早期应用麦克马洪评分评估急性肾损伤风险,早期启动肾脏替代治疗及肾脏保护治疗。在重症患者中,早期使用包括喹诺酮类在内的经验性抗生素可能改善预后。