Park Yong Suk, Yoon Hee, Kang Soo Yeon, Jo Ik Joon, Woo Sookyoung, Lee Guntak, Park Jong Eun, Kim Taerim, Lee Se Uk, Hwang Sung Yeon, Cha Won Chul, Shin Tae Gun
Department of Emergency Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, Korea.
Biomedical Statistics Center, Data Science Research Institute, Research Institute for Future Medicine, Samsung Medical Center, Seoul 06351, Korea.
Diagnostics (Basel). 2022 Mar 16;12(3):721. doi: 10.3390/diagnostics12030721.
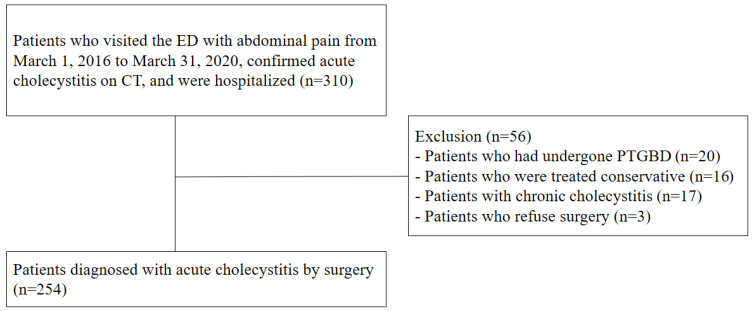
This study aimed to evaluate the diagnostic value of gallbladder width measurement with computed tomography (CT) in patients with acute cholecystitis. This retrospective case−control study was conducted between March 2016 and March 2020 at a tertiary emergency department. Of 310 patients, 254 patients with acute cholecystitis confirmed by surgery were compared with 254 patients diagnosed with other diseases (controls). In the acute cholecystitis group, the number of older patients with underlying illnesses was much higher (64% of men). Upon CT, the median (interquartile range [IQR]) gallbladder width was significantly longer in patients with acute cholecystitis (2.26 [1.82−2.78] cm vs. 3.73 [3.32−4.16] cm, p < 0.001). The optimal cut-off value of gallbladder width for differentiating acute cholecystitis was 3.12 cm, showing a sensitivity of 88% and specificity of 86%. In a multivariable analysis using a logistic regression model for diagnosing acute cholecystitis with CT findings (gallbladder width, length, stone, wall thickening, and pericholecystic fluid), a gallbladder width of ≥3.12 cm was significantly meaningful, even when adjusting for other variables (odds ratio 37.9; p < 0.001). Therefore, an increase in gallbladder width (≥3.12 cm) measured with CT can be a simple and sensitive diagnostic sign of acute cholecystitis, supporting the underlying pathophysiology of bile outflow obstruction.
本研究旨在评估计算机断层扫描(CT)测量胆囊宽度对急性胆囊炎患者的诊断价值。这项回顾性病例对照研究于2016年3月至2020年3月在一家三级急诊科进行。在310例患者中,将254例经手术确诊的急性胆囊炎患者与254例诊断为其他疾病的患者(对照组)进行比较。在急性胆囊炎组中,有基础疾病的老年患者数量多得多(男性占64%)。CT检查时,急性胆囊炎患者的胆囊宽度中位数(四分位间距[IQR])明显更长(2.26[1.82 - 2.78]cm对3.73[3.32 - 4.16]cm,p<0.001)。鉴别急性胆囊炎的胆囊宽度最佳截断值为3.12cm,敏感性为88%,特异性为86%。在使用逻辑回归模型对CT表现(胆囊宽度、长度、结石、胆囊壁增厚和胆囊周围积液)诊断急性胆囊炎进行多变量分析时,即使对其他变量进行调整,胆囊宽度≥3.12cm仍具有显著意义(比值比37.9;p<0.001)。因此,CT测量的胆囊宽度增加(≥3.12cm)可作为急性胆囊炎的一个简单且敏感的诊断标志,支持胆汁流出受阻的潜在病理生理学机制。