Turner Institute for Brain and Mental Health, Monash University, Clayton, Victoria, Australia.
Harvard T.H. Chan School of Public Health, Harvard University, Boston, Massachusetts.
JAMA Netw Open. 2022 Mar 1;5(3):e224071. doi: 10.1001/jamanetworkopen.2022.4071.
Up to 40% of dementia cases are potentially preventable; therefore, it is important to identify high-risk groups to whom resources could be targeted for maximal impact in preventing late-life dementia. The association of neighborhood-level socioeconomic status (SES) with cognition and dementia risk is not well known, particularly in midlife when late-life dementia may still be preventable through established interventions, such as blood pressure management.
To examine whether neighborhood-level SES is associated with differences in cognitive performance and dementia risk scores.
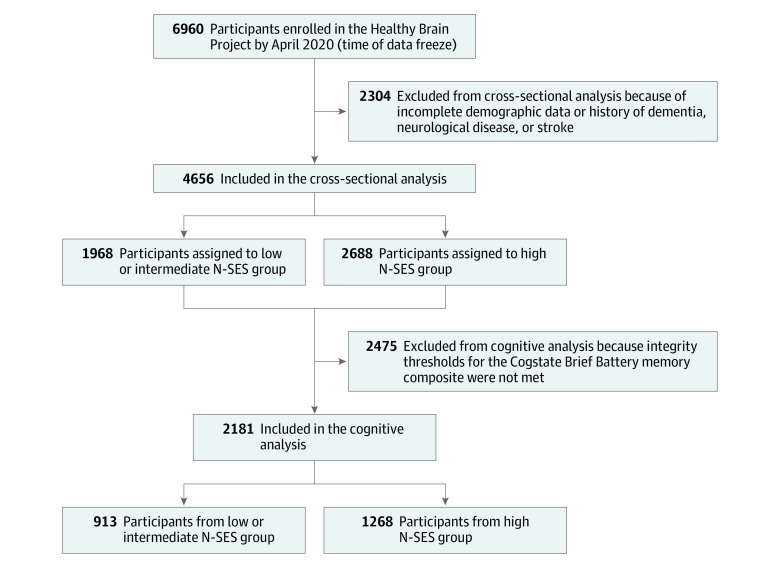
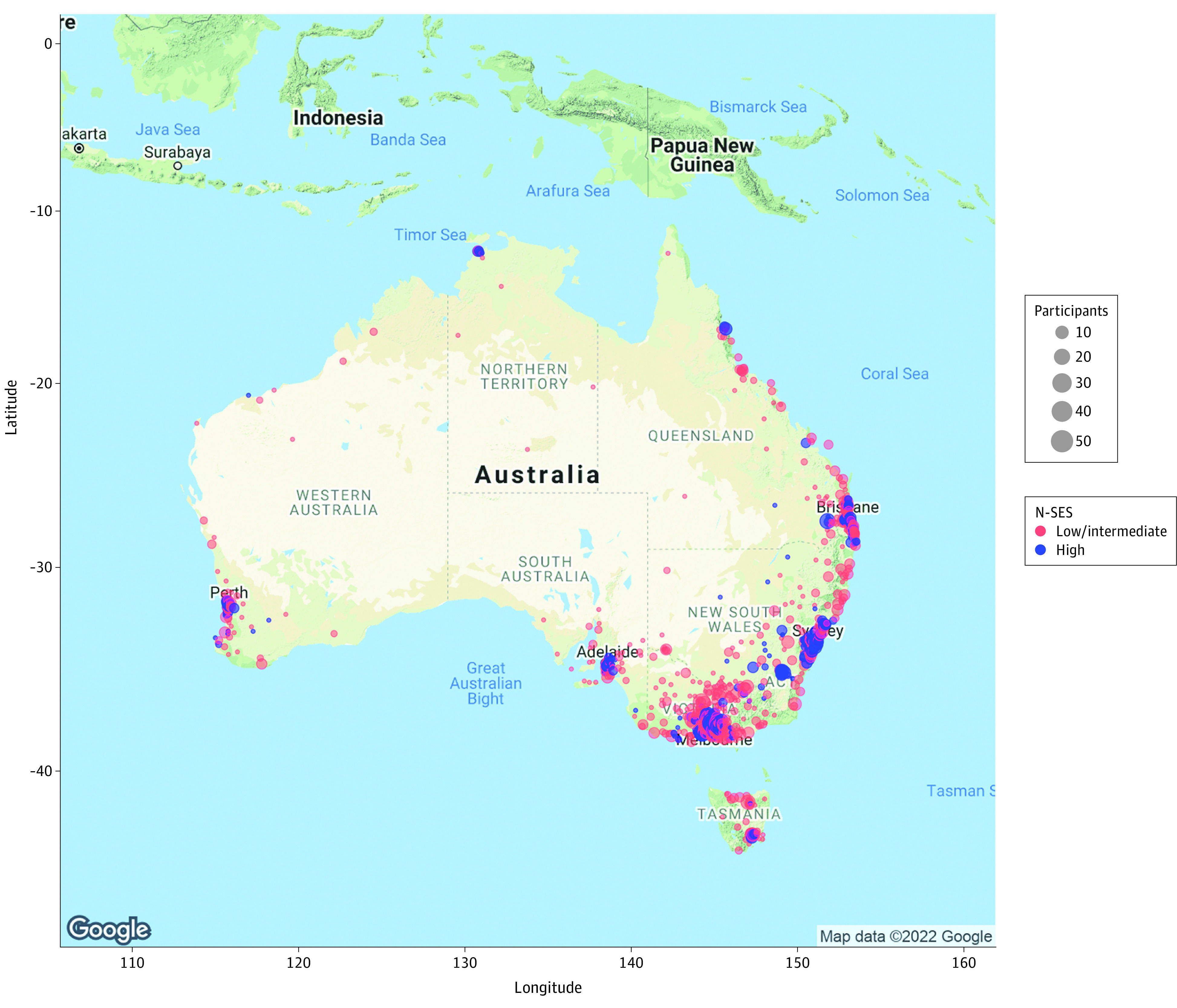
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study analyzed data collected between November 17, 2016, and April 14, 2020, from 4656 participants in the longitudinal population-based Healthy Brain Project cohort. This large online cohort comprised community-dwelling individuals geographically dispersed across Australia. Participants were aged 40 to 70 years without dementia or other major neurological conditions.
Neighborhood-level SES was computed by matching participants' residential addresses to the Australian Bureau of Statistics Index of Relative Socio-economic Advantage and Disadvantage (IRSAD). Postcodes provided by each participant were used to derive an IRSAD score that ranked participants according to deciles of neighborhood-level SES (range, 1-10, with higher deciles indicating greater socioeconomic advantage); neighborhoods in deciles 1 to 7 were considered to have low or intermediate SES, and neighborhoods in deciles 8 to 10 were considered to have high SES.
Dementia risk estimated using the dementia risk score from the Cardiovascular Risk Factors, Aging, and Incidence of Dementia (CAIDE) tool (n = 4656) and cognitive composite scores for memory and attention measured by the Cogstate Brief Battery (n = 2181).
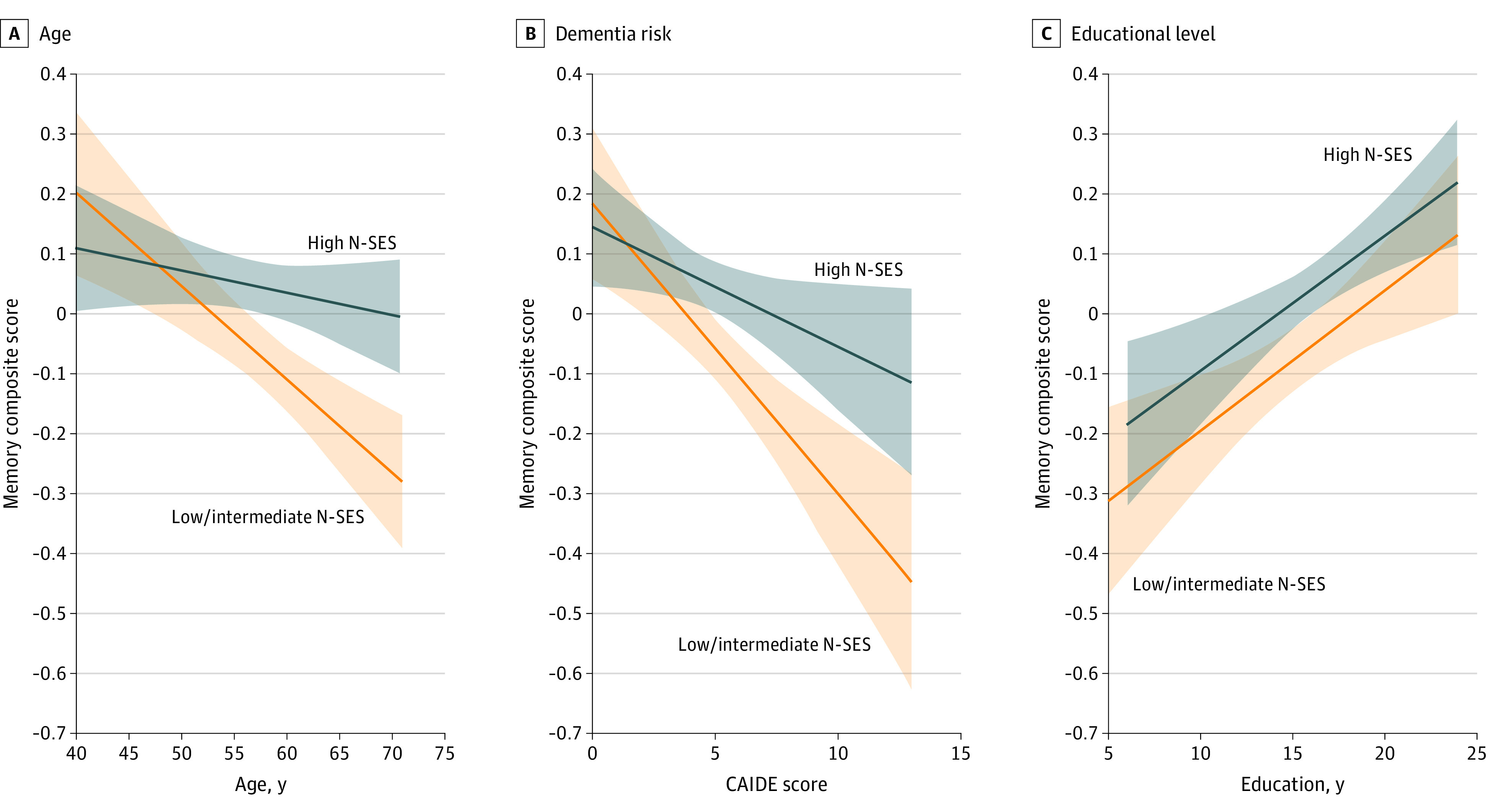
Of 4656 participants (mean [SD] age, 56.1 [7.2] years; 3445 women [74.0%]), 2688 individuals (57.7%) lived in areas with high neighborhood-level SES (IRSAD decile ≥8), and 1968 (42.3%) lived in areas with low or intermediate neighborhood-level SES (IRSAD decile <8), with 1263 individuals (27.1%) residing in rural or regional areas. A total of 6 participants (0.1%) identified as African, 121 (2.6%) as Asian, 57 (1.2%) as Indigenous Australian, 24 (0.5%) as Latin American, 9 (0.2%) as Pacific Islander, 3671 (78.8%) as White or European, and 768 (16.5%) indicated other race (not specified). Each decile unit increase in neighborhood-level SES was associated with a lower CAIDE dementia risk score after adjustment for race and rurality (β [SE] = -0.070 [0.019]; P = .004). Each decile unit increase was also associated with better memory (β [SE] = 0.022 [0.006]; P = .006) but not with better attention (β [SE] = 0.009 [0.007]; P = .34), as measured by Cogstate Brief Battery composite z scores after adjustment for age, sex, race, years of education, and rurality. When comparing memory performance between individuals with IRSAD scores higher and lower than decile 8, neighborhood-level SES interacted with age (F1-2171 = 6.33; P = .02) and CAIDE dementia risk scores (F1-2173 = 4.02; P = .08). Differences in memory between neighborhood-level SES categories were larger among participants who were older and had a higher risk of dementia.
In this study, higher neighborhood-level SES was associated with better memory and lower dementia risk scores. These results suggest that efforts to lower dementia risk factors in disadvantaged areas are needed to curtail the increasing burden of dementia and that inclusion of individuals living in areas with lower SES in research on dementia is warranted to improve understanding and potential interventions.
多达 40%的痴呆病例是可以预防的;因此,确定高危人群至关重要,以便在预防老年痴呆症方面投入最大的资源。目前尚不清楚邻里社会经济地位(SES)与认知和痴呆风险之间的关联,尤其是在中年时期,此时通过血压管理等既定干预措施,仍有可能预防晚年痴呆症。
研究邻里 SES 是否与认知表现和痴呆风险评分的差异有关。
设计、地点和参与者:本横断面研究分析了 2016 年 11 月 17 日至 2020 年 4 月 14 日期间从澳大利亚纵向基于人群的健康大脑计划队列中 4656 名参与者的数据。该大型在线队列由居住在澳大利亚各地的社区居民组成。参与者年龄在 40 至 70 岁之间,没有痴呆或其他主要神经疾病。
通过将参与者的居住地址与澳大利亚统计局相对社会经济优势和劣势指数(IRSAD)相匹配,计算邻里 SES。每位参与者提供的邮政编码用于得出 IRSAD 评分,根据邻里 SES 的十分位数(范围为 1-10,高分位数表示社会经济优势更大)对参与者进行排名;十分位数 1 至 7 的社区被认为具有较低或中等 SES,十分位数 8 至 10 的社区被认为具有较高 SES。
使用心血管风险因素、衰老和痴呆发生率(CAIDE)工具的痴呆风险评分(n=4656)和 Cogstate 简短电池的记忆和注意力认知复合评分(n=2181)估计痴呆风险。
在 4656 名参与者中(平均[标准差]年龄,56.1[7.2]岁;3445 名女性[74.0%]),2688 人(57.7%)居住在 SES 较高的地区(IRSAD 十分位数≥8),1968 人(42.3%)居住在 SES 较低或中等的地区(IRSAD 十分位数<8),1263 人(27.1%)居住在农村或偏远地区。6 名参与者(0.1%)认定为非洲人,121 名参与者(2.6%)认定为亚洲人,57 名参与者(1.2%)认定为澳大利亚原住民,24 名参与者(0.5%)认定为拉丁美洲人,9 名参与者(0.2%)认定为太平洋岛民,3671 名参与者(78.8%)认定为白种人或欧洲人,768 名参与者(16.5%)表示其他种族(未指定)。调整种族和农村情况后,SES 每增加十分位,CAIDE 痴呆风险评分就会降低(β[SE]=-0.070[0.019];P=0.004)。SES 每增加十分位,记忆力也会更好(β[SE]=0.022[0.006];P=0.006),但注意力(β[SE]=0.009[0.007];P=0.34)不会更好,这是根据 Cogstate 简短电池复合 z 评分衡量的,调整了年龄、性别、种族、受教育年限和农村情况。当比较 IRSAD 评分高于和低于 8 分的个体的记忆表现时,SES 与年龄(F1-2171=6.33;P=0.02)和 CAIDE 痴呆风险评分(F1-2173=4.02;P=0.08)之间存在交互作用。在年龄较大和痴呆风险较高的参与者中,SES 类别之间的记忆差异更大。
在这项研究中,较高的邻里 SES 与更好的记忆力和较低的痴呆风险评分相关。这些结果表明,需要在弱势地区努力降低痴呆风险因素,以遏制痴呆症负担的不断增加,并且有必要将居住在 SES 较低地区的个人纳入痴呆症研究,以提高对痴呆症的认识和潜在干预措施。