Division of Hepato-Pancreato-Biliary Surgery, Department of Surgery, Johns Hopkins University School of Medicine, Baltimore, Maryland.
Department of Abdominal Surgery, Helsinki University Hospital, Helsinki, Finland.
Clin Cancer Res. 2022 Aug 2;28(15):3296-3307. doi: 10.1158/1078-0432.CCR-21-4165.
Patient-derived organoids (PDO) are a promising technology to support precision medicine initiatives for patients with pancreatic ductal adenocarcinoma (PDAC). PDOs may improve clinical next-generation sequencing (NGS) and enable rapid ex vivo chemotherapeutic screening (pharmacotyping).
PDOs were derived from tissues obtained during surgical resection and endoscopic biopsies and studied with NGS and pharmacotyping. PDO-specific pharmacotype is assessed prospectively as a predictive biomarker of clinical therapeutic response by leveraging data from a randomized controlled clinical trial.
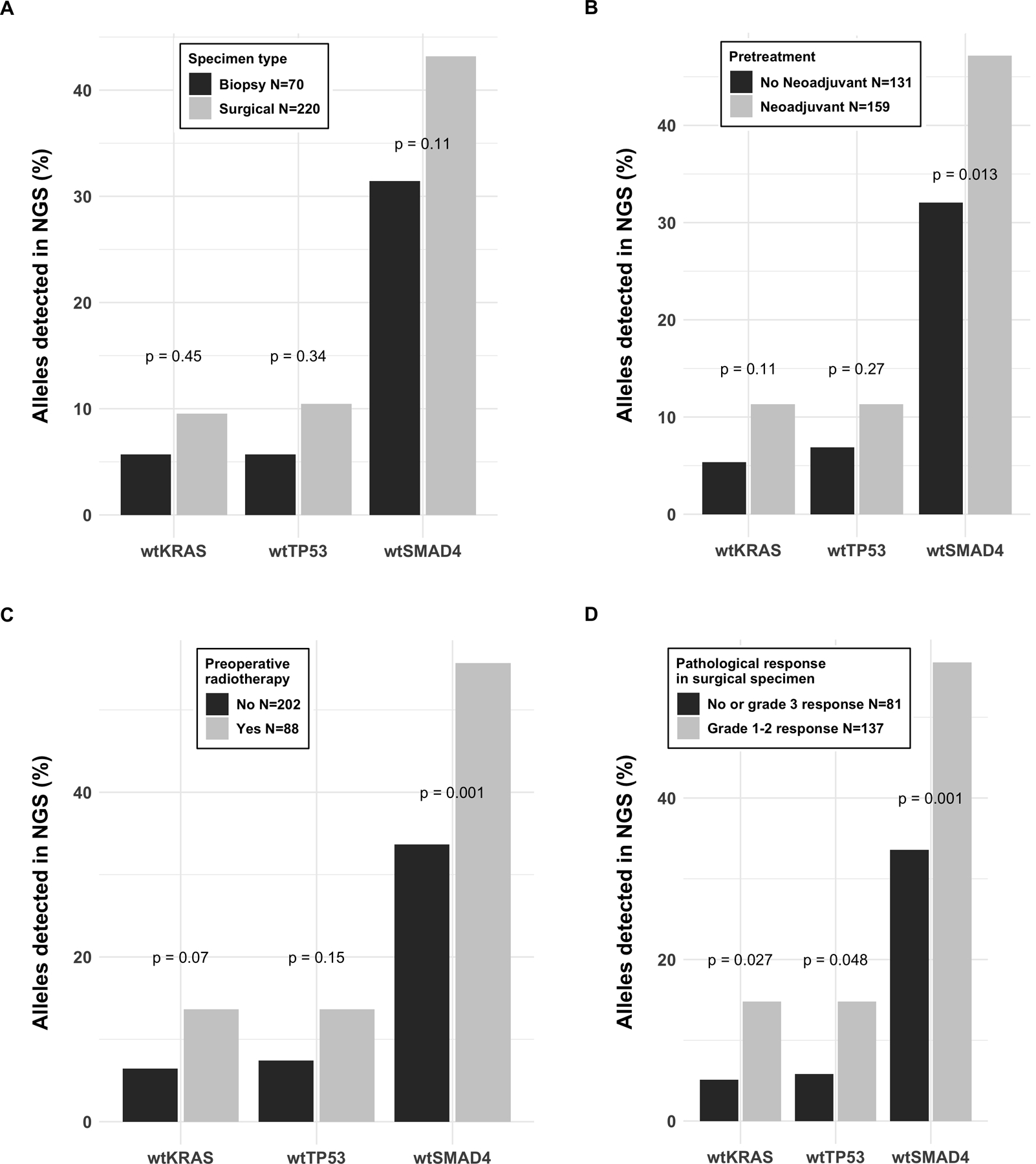
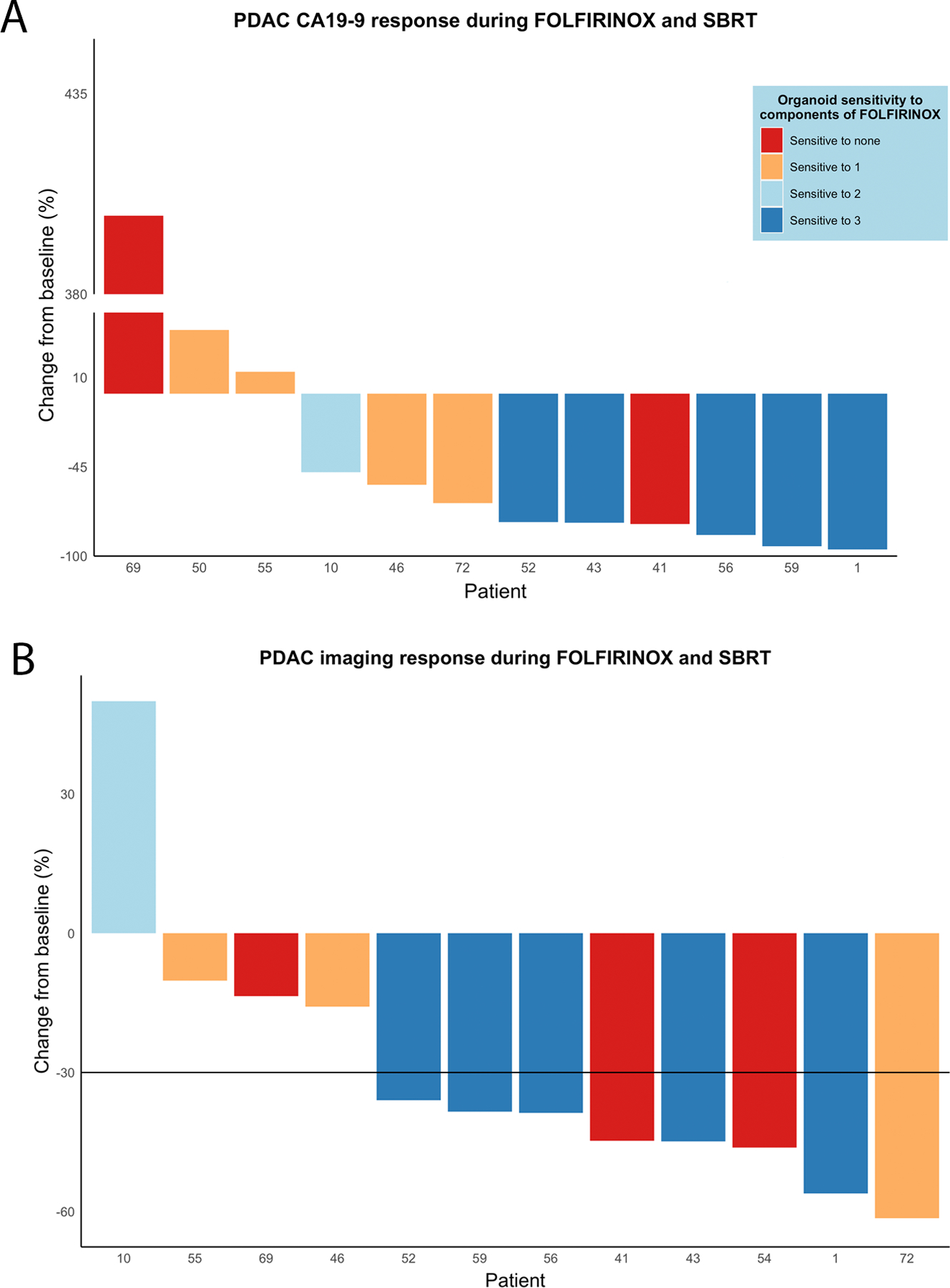
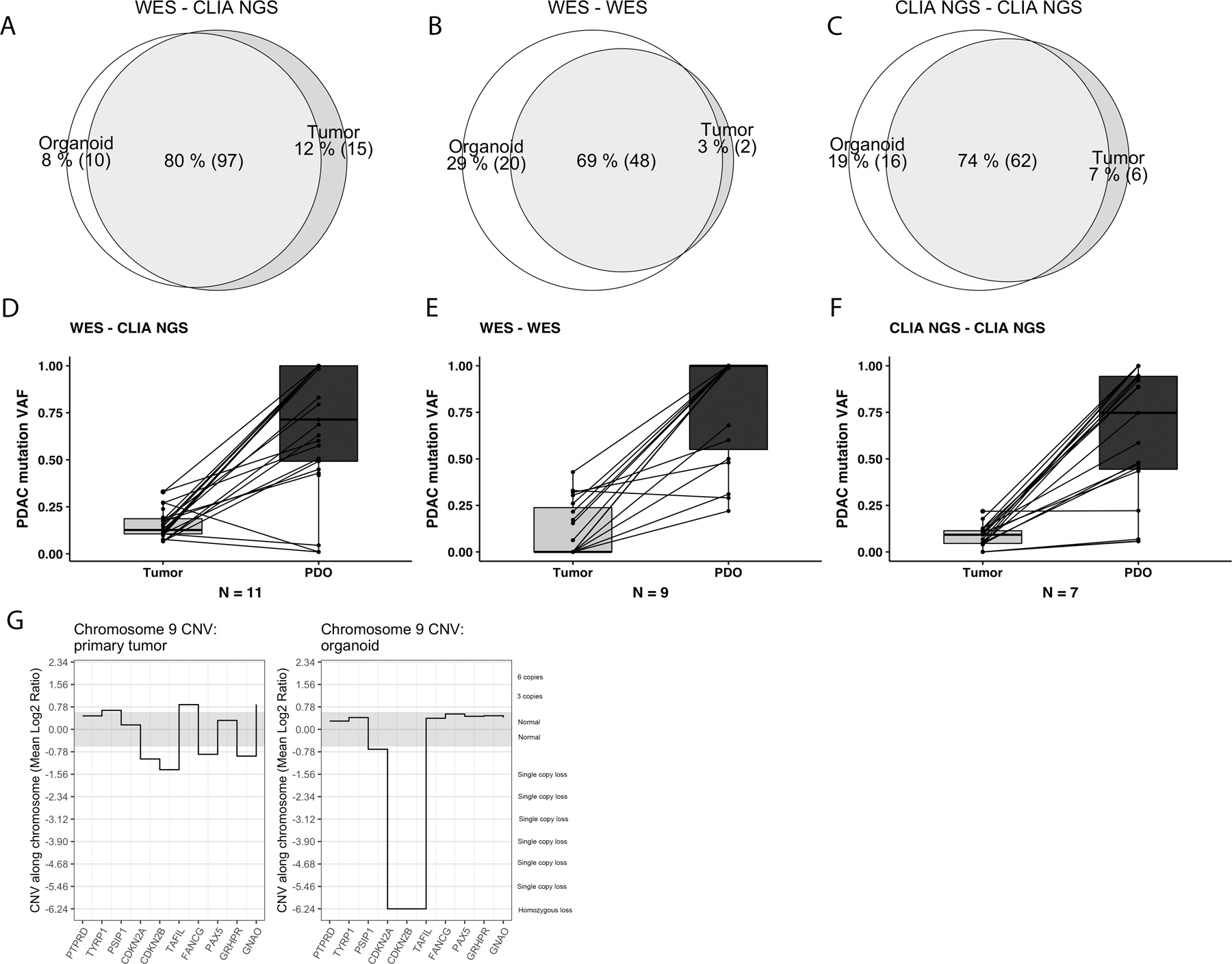
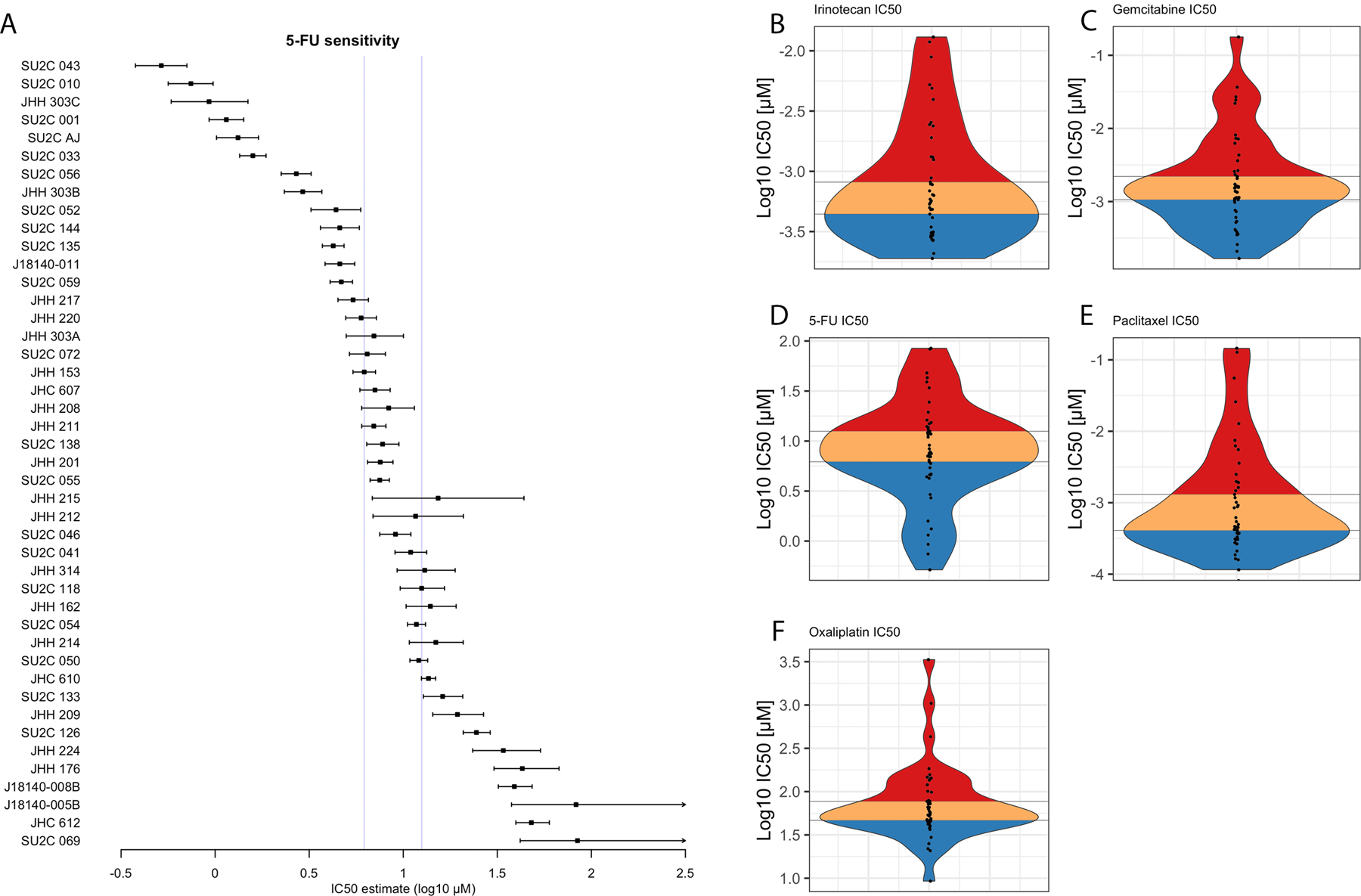
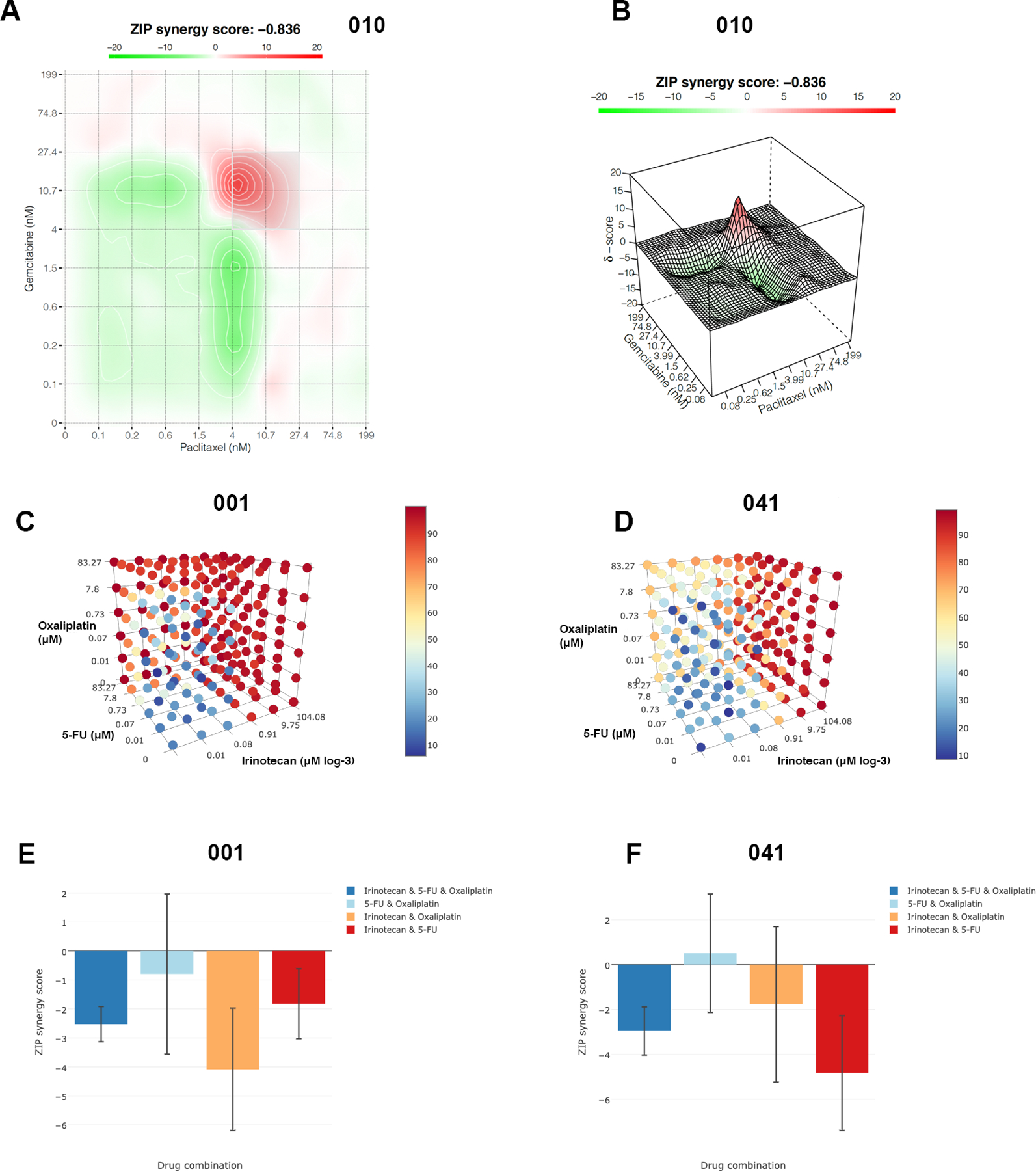
Clinical sequencing pipelines often fail to detect PDAC-associated somatic mutations in surgical specimens that demonstrate a good pathologic response to previously administered chemotherapy. Sequencing the PDOs derived from these surgical specimens, after biomass expansion, improves the detection of somatic mutations and enables quantification of copy number variants. The detection of clinically relevant mutations and structural variants is improved following PDO biomass expansion. On clinical trial, PDOs were derived from biopsies of treatment-naïve patients prior to treatment with FOLFIRINOX (FFX). Ex vivo PDO pharmacotyping with FFX components predicted clinical therapeutic response in these patients with borderline resectable or locally advanced PDAC treated in a neoadjuvant or induction paradigm. PDO pharmacotypes suggesting sensitivity to FFX components were associated with longitudinal declines of tumor marker, carbohydrate-antigen 19-9 (CA-19-9), and favorable RECIST imaging response.
PDOs established from tissues obtained from patients previously receiving cytotoxic chemotherapies can be accomplished in a clinically certified laboratory. Sequencing PDOs following biomass expansion improves clinical sequencing quality. High in vitro sensitivity to standard-of-care chemotherapeutics predicts good clinical response to systemic chemotherapy in PDAC. See related commentary by Zhang et al., p. 3176.
患者来源的类器官(PDO)是支持胰腺导管腺癌(PDAC)患者精准医学计划的一项有前途的技术。PDO 可改善临床下一代测序(NGS)并实现快速体外化疗筛选(药物代谢动力学)。
PDO 源自手术切除和内镜活检获得的组织,并通过 NGS 和药物代谢动力学进行研究。通过利用来自随机对照临床试验的数据,前瞻性地评估 PDO 特异性药物代谢动力学作为临床治疗反应的预测生物标志物。
临床测序方案通常无法检测到手术标本中与 PDAC 相关的体细胞突变,这些标本对先前给予的化疗反应良好。对这些手术标本进行生物量扩增后衍生的 PDO 进行测序,可以提高体细胞突变的检测,并能够定量分析拷贝数变异。PDO 生物量扩增后,临床相关突变和结构变异的检测得到改善。在临床试验中,PDO 是从接受 FOLFIRINOX(FFX)治疗的治疗初治患者的活检中衍生而来的。用 FFX 成分对 PDO 进行体外药物代谢动力学预测,对接受新辅助或诱导治疗的边界可切除或局部晚期 PDAC 患者具有临床治疗反应。对 FFX 成分敏感的 PDO 药物代谢动力学与肿瘤标志物、碳水化合物抗原 19-9(CA-19-9)的纵向下降以及有利的 RECIST 成像反应相关。
可以在临床认证的实验室中完成从先前接受细胞毒性化疗的患者获得的组织中建立的 PDO。生物量扩增后对 PDO 进行测序可提高临床测序质量。对标准治疗化疗药物的高体外敏感性可预测 PDAC 患者对全身化疗的良好临床反应。请参阅相关评论文章,第 3176 页,由 Zhang 等人撰写。