Fifth Department of Medicine, University Hospital Mannheim, Heidelberg University, Mannheim, Germany.
Department of Personalized Oncology, University Hospital Mannheim, Heidelberg University, Mannheim, Germany.
Invest New Drugs. 2022 Aug;40(4):798-809. doi: 10.1007/s10637-022-01227-5. Epub 2022 Apr 7.
Previous research focused on the clinical evidence supporting new cancer drugs' initial US Food and Drug Administration (FDA) approval. However, targeted drugs are increasingly approved for supplementary indications of unknown evidence and benefit.
To examine the clinical trial evidence supporting new targeted cancer drugs' initial and supplementary indication approval in the US, EU, Canada, and Australia.
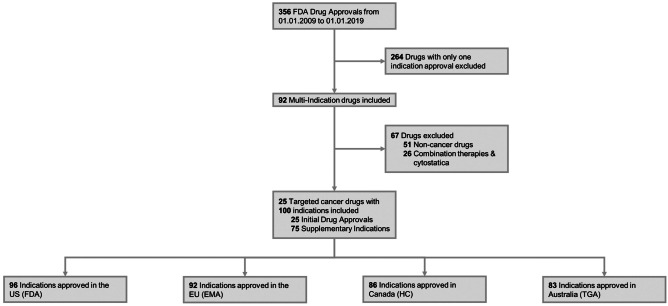
25 cancer drugs across 100 indications were identified with FDA approval between 2009-2019. Data on regulatory approval and clinical trials were extracted from the FDA, European Medicines Agency (EMA), Health Canada (HC), Australian Therapeutic Goods Administration (TGA), and clinicaltrials.gov. Regional variations were compared with χ-tests. Multivariate logistic regressions compared characteristics of initial and supplementary indication approvals, reporting adjusted odds ratios (AOR) with 95% confidence intervals (CI).
Out of 100 considered cancer indications, the FDA approved 96, the EMA 92, HC 86, and the TGA 83 (83%, p < 0.05). The FDA more frequently granted priority review, conditional approval, and orphan designations than other agencies. Initial approvals were more likely to receive conditional / accelerated approval (AOR: 2.69, 95%CI [1.07-6.77], p < 0.05), an orphan designation (AOR: 3.32, 95%CI [1.38-8.00], p < 0.01), be under priority review (AOR: 2.60, 95%CI [1.17-5.78], p < 0.05), and be monotherapies (AOR: 5.91, 95%CI [1.14-30.65], p < 0.05) than supplementary indications. Initial indications' pivotal trials tended to be shorter (AOR per month: 0.96, 95%CI [0.93-0.99], p < 0.05), of lower phase design (AOR per clinical phase: 0.28, 95%CI [0.09-0.85], p < 0.05), and enroll more patients (AOR per 100 patients: 1.19, 95%CI [1.01-1.39], p < 0.05).
Targeted cancer drugs are increasingly approved for multiple indications of varying clinical benefit. Drugs are first approved as monotherapies in rare diseases with a high unmet need. Whilst expedited regulatory review incentivizes this prioritization, indication-specific safety, efficacy, and pricing policies are necessary to reflect each indication's differential clinical and economic value.
先前的研究主要关注支持新抗癌药物在美国食品药品监督管理局(FDA)首次批准的临床证据。然而,靶向药物越来越多地被批准用于具有未知证据和获益的补充适应证。
在美国、欧盟、加拿大和澳大利亚,考察新靶向抗癌药物首次和补充适应证批准的临床试验证据。
2009-2019 年期间,FDA 批准了 100 种适应证的 25 种抗癌药物。从 FDA、欧洲药品管理局(EMA)、加拿大卫生部(HC)、澳大利亚治疗用品管理局(TGA)和 clinicaltrials.gov 提取监管批准和临床试验数据。采用 χ 检验比较区域差异。采用多变量逻辑回归比较初始和补充适应证批准的特征,报告调整后的优势比(AOR)及其 95%置信区间(CI)。
100 种考虑的癌症适应证中,FDA 批准了 96 种,EMA 批准了 92 种,HC 批准了 86 种,TGA 批准了 83 种(83%,p<0.05)。与其他机构相比,FDA 更频繁地授予优先审查、有条件批准和孤儿药认定。初始批准更有可能获得有条件/加速批准(AOR:2.69,95%CI [1.07-6.77],p<0.05)、孤儿药认定(AOR:3.32,95%CI [1.38-8.00],p<0.01)、优先审查(AOR:2.60,95%CI [1.17-5.78],p<0.05)和单药治疗(AOR:5.91,95%CI [1.14-30.65],p<0.05),而补充适应证则不然。初始适应证的关键性试验往往时间较短(AOR 每月:0.96,95%CI [0.93-0.99],p<0.05)、设计阶段较低(AOR 每临床阶段:0.28,95%CI [0.09-0.85],p<0.05),且纳入的患者更多(AOR 每 100 名患者:1.19,95%CI [1.01-1.39],p<0.05)。
靶向抗癌药物越来越多地被批准用于具有不同临床获益的多种适应证。药物最初作为单一疗法用于罕见疾病,这些疾病存在着巨大的未满足的医疗需求。虽然加快监管审查会激励这种优先级排序,但需要制定针对适应证的安全性、疗效和定价政策,以反映每个适应证的差异临床和经济价值。