Cammarota Gianmaria, Simonte Rachele, De Robertis Edoardo
Dipartimento di Medicina e Chirurgia, Università degli Studi di Perugia, Perugia, Italy.
Front Med (Lausanne). 2022 Mar 24;9:874250. doi: 10.3389/fmed.2022.874250. eCollection 2022.
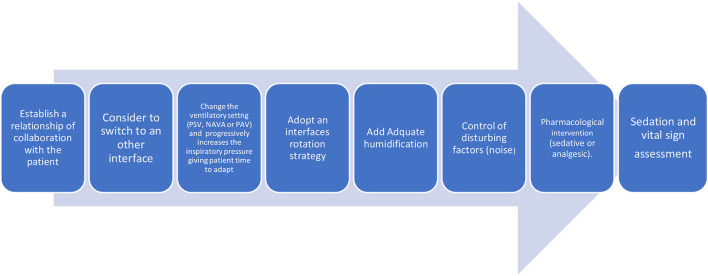
Non-invasive ventilation (NIV) has been shown to be effective in avoiding intubation and improving survival in patients with acute hypoxemic respiratory failure (ARF) when compared to conventional oxygen therapy. However, NIV is associated with high failure rates due, in most cases, to patient discomfort. Therefore, increasing attention has been paid to all those interventions aimed at enhancing patient's tolerance to NIV. Several practical aspects have been considered to improve patient adaptation. In particular, the choice of the interface and the ventilatory setting adopted for NIV play a key role in the success of respiratory assistance. Among the different NIV interfaces, tolerance is poorest for the nasal and oronasal masks, while helmet appears to be better tolerated, resulting in longer use and lower NIV failure rates. The choice of fixing system also significantly affects patient comfort due to pain and possible pressure ulcers related to the device. The ventilatory setting adopted for NIV is associated with varying degrees of patient comfort: patients are more comfortable with pressure-support ventilation (PSV) than controlled ventilation. Furthermore, the use of electrical activity of the diaphragm (EADi)-driven ventilation has been demonstrated to improve patient comfort when compared to PSV, while reducing neural drive and effort. If non-pharmacological remedies fail, sedation can be employed to improve patient's tolerance to NIV. Sedation facilitates ventilation, reduces anxiety, promotes sleep, and modulates physiological responses to stress. Judicious use of sedation may be an option to increase the chances of success in some patients at risk for intubation because of NIV intolerance consequent to pain, discomfort, claustrophobia, or agitation. During the Coronavirus Disease-19 (COVID-19) pandemic, NIV has been extensively employed to face off the massive request for ventilatory assistance. Prone positioning in non-intubated awake COVID-19 patients may improve oxygenation, reduce work of breathing, and, possibly, prevent intubation. Despite these advantages, maintaining prone position can be particularly challenging because poor comfort has been described as the main cause of prone position discontinuation. In conclusion, comfort is one of the major determinants of NIV success. All the strategies aimed to increase comfort during NIV should be pursued.
与传统氧疗相比,无创通气(NIV)已被证明在避免急性低氧性呼吸衰竭(ARF)患者插管和提高生存率方面有效。然而,NIV与高失败率相关,在大多数情况下,原因是患者不适。因此,人们越来越关注所有旨在提高患者对NIV耐受性的干预措施。为改善患者适应性,已考虑了几个实际方面。特别是,NIV所采用的接口和通气设置在呼吸辅助的成功中起着关键作用。在不同的NIV接口中,鼻罩和口鼻面罩的耐受性最差,而头盔似乎耐受性更好,使用时间更长且NIV失败率更低。固定系统的选择也会因与设备相关的疼痛和可能的压疮而显著影响患者舒适度。NIV所采用的通气设置与不同程度的患者舒适度相关:患者对压力支持通气(PSV)比对控制通气更舒适。此外,与PSV相比,使用膈肌电活动(EADi)驱动通气已被证明可提高患者舒适度,同时减少神经驱动和用力。如果非药物治疗无效,可采用镇静来提高患者对NIV的耐受性。镇静有助于通气、减轻焦虑、促进睡眠并调节对压力的生理反应。明智地使用镇静可能是增加一些因疼痛、不适、幽闭恐惧症或躁动导致NIV不耐受而有插管风险患者成功几率的一种选择。在冠状病毒病2019(COVID - 19)大流行期间,NIV已被广泛用于应对大量的通气辅助需求。非插管清醒COVID - 19患者的俯卧位可能改善氧合、减少呼吸功,并可能防止插管。尽管有这些优点,但保持俯卧位可能特别具有挑战性,因为舒适度差被描述为俯卧位中断的主要原因。总之,舒适度是NIV成功的主要决定因素之一。应采取所有旨在提高NIV期间舒适度的策略。