Division of Occupational and Environmental Medicine, Institute of Laboratory Medicine, Lund University, SE-223 83 Lund, Sweden.
Centre for Health Equity Studies (CHESS), Department of Public Health Sciences, Stockholm University, SE-114 19 Stockholm, Sweden.
Int J Environ Res Public Health. 2022 Mar 30;19(7):4080. doi: 10.3390/ijerph19074080.
To investigate the association between socio-economic factors and the risk of preeclampsia in Sweden, specifically investigating if this relationship is confounded by maternal region of birth.
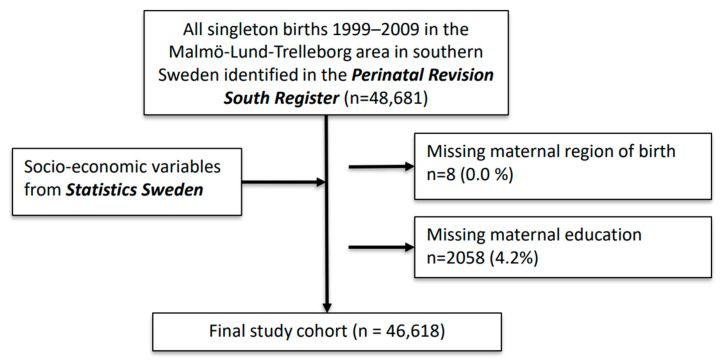
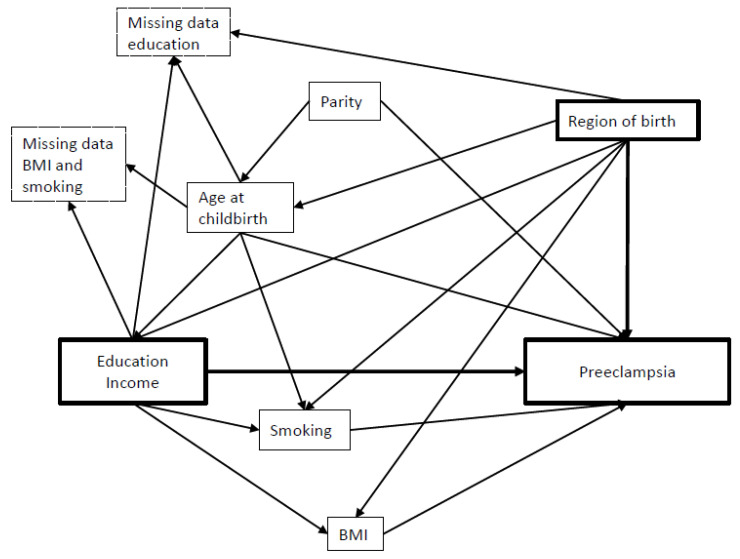
All singleton births between 1999 and 2009 in an ethnically diverse area in southern Sweden, totaling 46,618 pregnancies, were included in this study. The data on maternal pregnancy outcomes were retrieved from a regional birth register and socio-economic variables from Statistics Sweden. The risk ratios for preeclampsia were calculated for educational level and household disposable income, adjusting for maternal region of birth, maternal age, body mass index, parity, and smoking.
Low income levels were associated with a higher risk for preeclampsia, adjusted risk ratio (aRR) = 1.25 (95% confidence interval [CI]: 0.99, 1.59) and aRR = 1.36 (95% CI: 1.10, 1.68) for the two lowest quintiles, respectively, compared to the highest. There was an educational gradient in preeclampsia risk, although not all categories reached statistical significance: aRR = 1.16, (95% CI: 0.89-1.50) for low educational attainment and aRR = 1.23 (95% CI: 1.08, 1.41) for intermediate educational attainment compared to women with highest education. The socio-economic gradient remained after adjusting for region of birth. There was a lower risk for preeclampsia for women born in Asia, aRR = 0.60 (95% CI: 0.47, 0.75), regardless of socio-economic position.
An increased risk for preeclampsia was seen for women with measures of lower socio-economic position, even in a universal, government-funded healthcare setting. The relationship was not explained by region of birth, indicating that the excess risk is not due to ethnically differential genetic pre-disposition but rather due to modifiable factors.
在瑞典研究社会经济因素与子痫前期风险之间的关联,具体探讨这种关联是否受到产妇出生地的影响。
本研究纳入了瑞典南部一个种族多样化地区 1999 年至 2009 年间所有的单胎妊娠,共 46618 例妊娠。产妇妊娠结局数据来自区域出生登记处,社会经济变量数据来自瑞典统计局。调整了产妇出生地、产妇年龄、体重指数、产次和吸烟状况后,计算了子痫前期的教育水平和家庭可支配收入的风险比。
与收入最高组相比,低收入水平与子痫前期风险增加相关,最低两个五分位数的调整风险比(aRR)分别为 1.25(95%置信区间 [CI]:0.99,1.59)和 1.36(95% CI:1.10,1.68);存在子痫前期风险的教育梯度,尽管并非所有类别均达到统计学意义:与教育程度最高的女性相比,低教育程度的 aRR 为 1.16(95% CI:0.89-1.50),中等教育程度的 aRR 为 1.23(95% CI:1.08,1.41)。调整出生地因素后,社会经济梯度仍然存在。与社会经济地位较高的女性相比,亚洲出生的女性子痫前期风险较低,aRR 为 0.60(95% CI:0.47,0.75)。
即使在全民享有政府资助的医疗保健的情况下,社会经济地位较低的女性子痫前期风险也会增加。这种关联不能用出生地来解释,这表明这种超额风险不是由于种族差异的遗传易感性,而是由于可改变的因素。