SW Thames Renal Unit, Epsom and St Helier University Hospitals NHS Trust, Epsom, UK.
Faculty of Medicine and Health Sciences, University of Nottingham, Nottingham, UK.
Trials. 2022 Apr 21;23(1):331. doi: 10.1186/s13063-022-06132-z.
Chronic kidney disease (CKD) is a very common long-term condition and powerful risk factor for cardiovascular disease (CVD). Low-dose aspirin is of proven benefit in the secondary prevention of myocardial infarction (MI) and stroke in people with pre-existing CVD. However, in people without CVD, the rates of MI and stroke are much lower, and the benefits of aspirin in the primary prevention of CVD are largely balanced by an increased risk of bleeding. People with CKD are at greatly increased risk of CVD and so the absolute benefits of aspirin are likely to be greater than in lower-risk groups, even if the relative benefits are the same. Post hoc evidence suggests the relative benefits may be greater in the CKD population but the risk of bleeding may also be higher. A definitive study of aspirin for primary prevention in this high-risk group, recommended by the National Institute for Health and Care Excellence (NICE) in 2014, has never been conducted. The question has global significance given the rising burden of CKD worldwide and the low cost of aspirin.
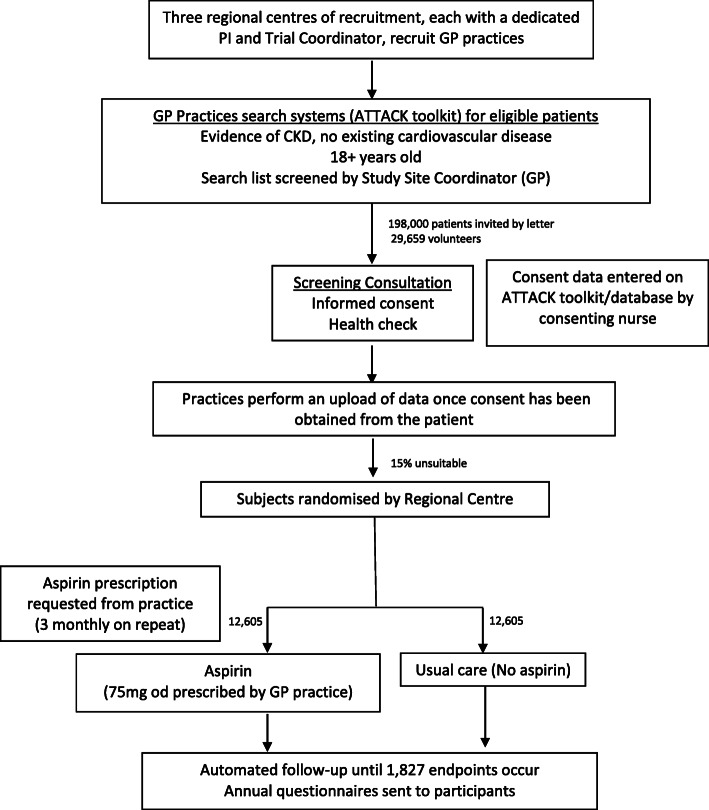
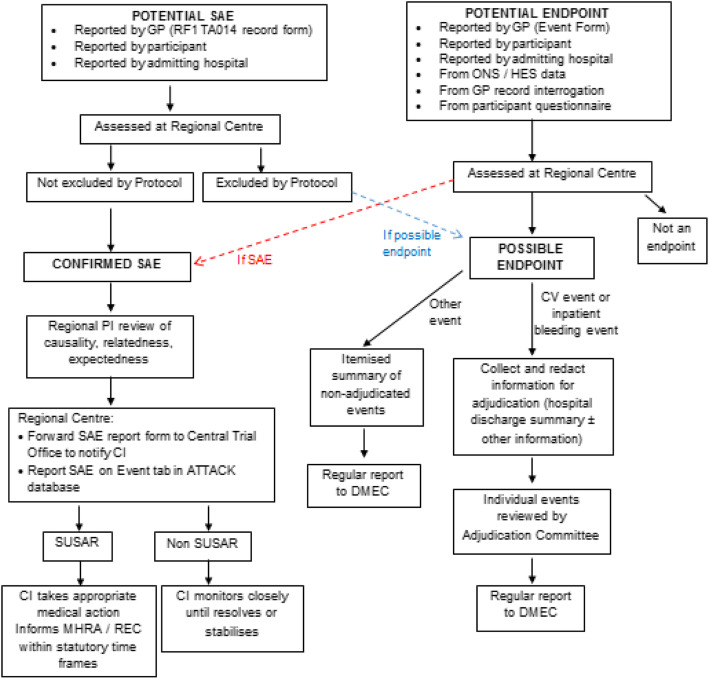
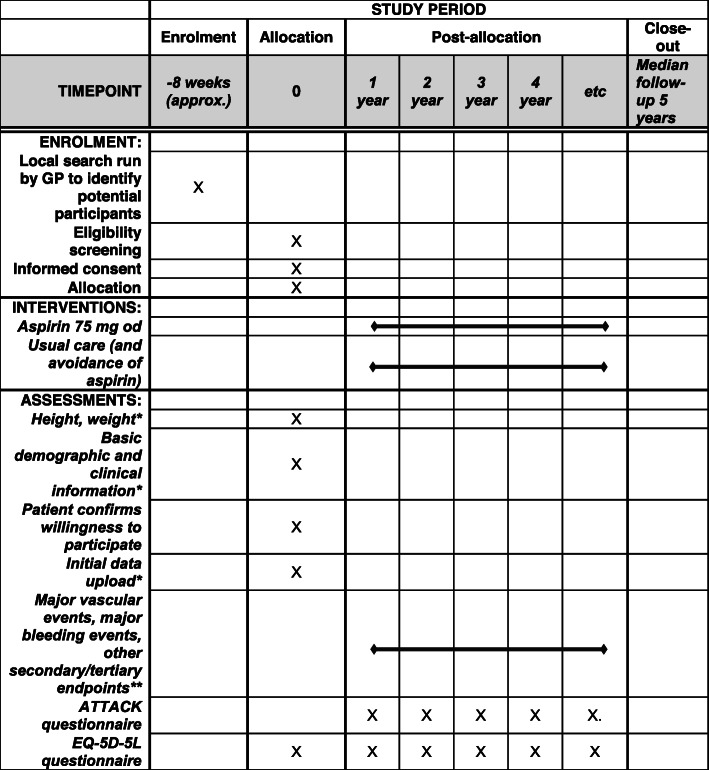
ATTACK is a pragmatic multicentre, prospective, randomised, open-label, blinded endpoint adjudication superiority trial of aspirin 75 mg daily vs. standard care for the primary prevention of CVD in 25,210 people aged 18 years and over with CKD recruited from UK Primary Care. Participants aged 18 years and over with CKD (GFR category G1-G4) will be identified in Primary Care and followed up using routinely collected data and annual questionnaires for an average of 5 years. The primary outcome is the time to first major vascular event (composite of non-fatal MI, non-fatal stroke and cardiovascular death [excluding confirmed intracranial haemorrhage and other fatal cardiovascular haemorrhage]). Deaths from other causes (including fatal bleeding) will be treated as competing events. The study will continue until 1827 major vascular events have occurred. The principal safety outcome is major intracranial and extracranial bleeding; this is hypothesised to be increased in those randomised to take aspirin. The key consideration is then whether and to what extent the benefits of aspirin from the expected reduction in CVD events exceed the risks of major bleeding.
This will be the first definitive trial of aspirin for primary CVD prevention in CKD patients. The research will be of great interest to clinicians, guideline groups and policy-makers, in the UK and globally, particularly given the high and rising prevalence of CKD that is driven by population ageing and epidemics of obesity and diabetes. The low cost of aspirin means that a positive result would be of relevance to low- and middle-income countries and the impact in the developed world less diluted by any inequalities in health care access.
ISRCTN: ISRCTN40920200 . EudraCT: 2018-000644-26 .
gov: NCT03796156.
慢性肾脏病(CKD)是一种非常常见的长期病症,也是心血管疾病(CVD)的强大风险因素。小剂量阿司匹林已被证明可有效预防已有 CVD 的人群发生心肌梗死(MI)和中风。然而,在没有 CVD 的人群中,MI 和中风的发生率要低得多,阿司匹林在 CVD 一级预防中的益处很大程度上被出血风险增加所抵消。CKD 患者 CVD 的风险大大增加,因此,即使相对益处相同,阿司匹林的绝对益处也可能大于低风险人群。事后证据表明,CKD 人群的相对益处可能更大,但出血风险也可能更高。鉴于全球范围内 CKD 负担的增加和阿司匹林的低成本,国家卫生与保健卓越研究所(NICE)于 2014 年建议对这一高危人群进行阿司匹林一级预防的确定性研究,但该研究从未进行过。鉴于全球范围内 CKD 的负担不断增加,且阿司匹林的成本低廉,该问题具有全球意义。
ATTACK 是一项在英国初级保健机构中招募的 25210 名年龄在 18 岁及以上 CKD 患者中进行的、针对阿司匹林 75mg 每日治疗与标准治疗在 CVD 一级预防中作用的实用、多中心、前瞻性、随机、开放标签、盲终点评估优效性试验。将在初级保健中发现年龄在 18 岁及以上的 CKD(GFR 1 至 4 期)患者,并通过常规收集的数据和每年的问卷调查进行随访,平均随访时间为 5 年。主要终点是首次主要血管事件(非致命性 MI、非致命性中风和心血管死亡的复合终点[不包括确认的颅内出血和其他致命性心血管出血])的时间。其他原因导致的死亡(包括致命性出血)将作为竞争事件处理。该研究将持续至发生 1827 例主要血管事件。主要安全性结局是主要颅内和颅外出血;假设阿司匹林治疗组出血风险增加。那么关键考虑因素是阿司匹林预防 CVD 事件的益处是否超过主要出血风险。
这将是第一项针对 CKD 患者 CVD 一级预防的阿司匹林的确定性研究。该研究将引起英国和全球临床医生、指南制定者和决策者的极大兴趣,特别是考虑到 CKD 的高患病率和不断上升,这是由人口老龄化以及肥胖和糖尿病的流行所驱动。阿司匹林的低成本意味着,阳性结果不仅对中低收入国家,而且对发达国家也具有重要意义,因为在这些国家,医疗保健获取方面的任何不平等都会使该结果的影响降低。
ISRCTN: ISRCTN40920200. EudraCT: 2018-000644-26.
gov: NCT03796156.