Laugesen Esben, Olesen Kevin K W, Peters Christian Daugaard, Buus Niels Henrik, Maeng Michael, Botker Hans Erik, Poulsen Per L
Department of Endocrinology and Internal Medicine Aarhus University Hospital Aarhus Denmark.
Regional Hospital Horsens Horsens Denmark.
J Am Heart Assoc. 2022 May 17;11(10):e025173. doi: 10.1161/JAHA.121.025173. Epub 2022 May 10.
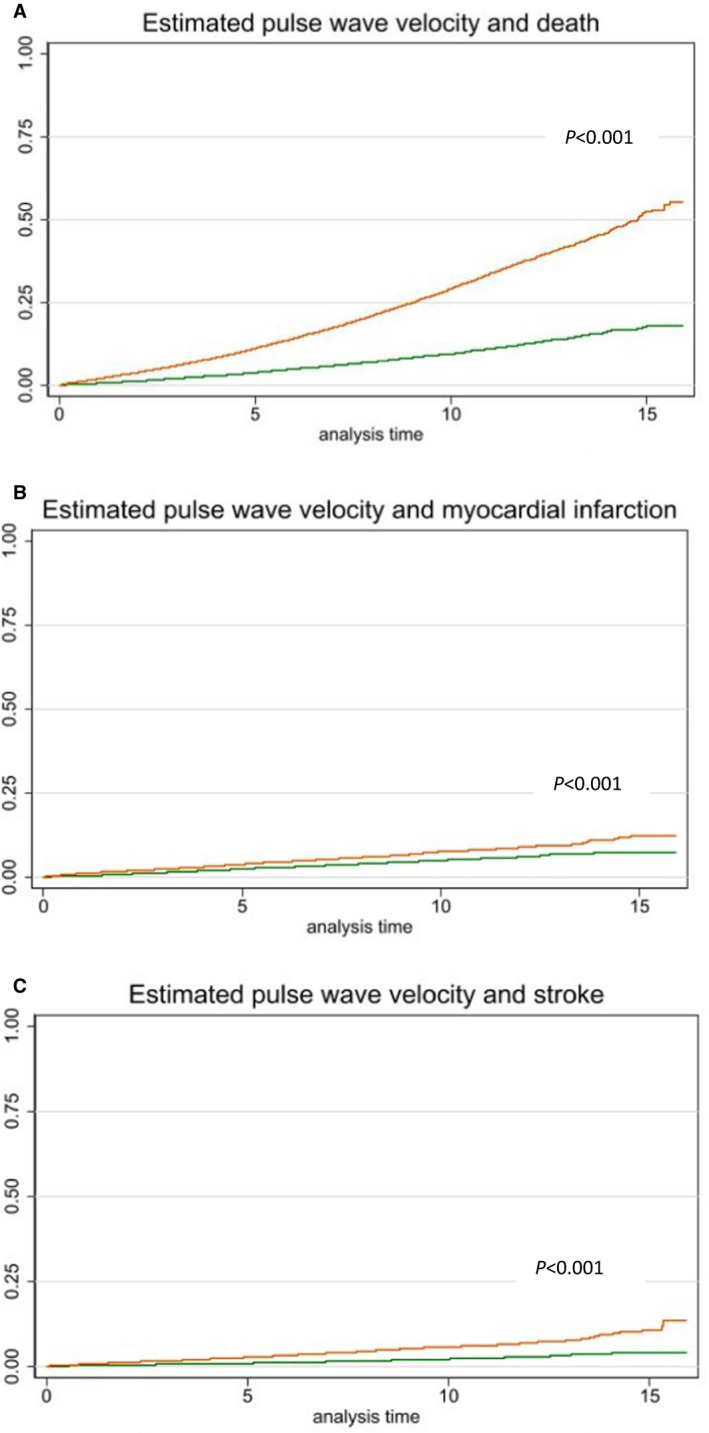
Background Estimated pulse wave velocity (ePWV) calculated by equations using age and blood pressure has been suggested as a new marker of mortality and cardiovascular risk. However, the prognostic potential of ePWV during long-term follow-up in patients with symptoms of stable angina remains unknown. Methods and Results In this study, ePWV was calculated in 25 066 patients without diabetes, previous myocardial infarction (MI), stroke, heart failure, or valvular disease (mean age 63.7±10.5 years, 58% male) with stable angina pectoris undergoing elective coronary angiography during 2003 to 2016. Multivariable Cox models were used to assess the association with incident all-cause mortality, MI, and stroke. Discrimination was assessed using Harrell´s C-index. During a median follow-up period of 8.5 years (interquartile range 5.5-11.3 years), 779 strokes, 1233 MIs, and 4112 deaths were recorded. ePWV was associated with all-cause mortality (hazard ratio [HR] per 1 m/s, 1.13; 95% CI, 1.05-1.21) and MI (HR per 1 m/s 1.23, 95% CI, 1.09-1.39) after adjusting for age, systolic blood pressure, body mass index, smoking, estimated glomerular filtration rate, Charlson Comorbidity Index score, antihypertensive treatment, statins, aspirin, and number of diseased coronary arteries. Compared with traditional risk factors, the adjusted model with ePWV was associated with a minor but likely not clinically relevant increase in discrimination for mortality, 76.63% with ePWV versus 76.56% without ePWV, <0.05. Conclusions In patients with stable angina pectoris, ePWV was associated with all-cause mortality and MI beyond traditional risk factors. However, the added prediction of mortality was not improved to a clinically relevant extent.
通过使用年龄和血压的方程计算得出的估计脉搏波速度(ePWV)已被提议作为死亡率和心血管风险的新标志物。然而,在稳定型心绞痛患者的长期随访中,ePWV的预后潜力仍不明确。
在本研究中,对2003年至2016年期间因稳定型心绞痛接受选择性冠状动脉造影的25066例无糖尿病、既往无心肌梗死(MI)、中风、心力衰竭或瓣膜疾病的患者(平均年龄63.7±10.5岁,58%为男性)计算ePWV。使用多变量Cox模型评估与全因死亡率、MI和中风事件的关联。使用Harrell´s C指数评估辨别力。在中位随访期8.5年(四分位间距5.5 - 11.3年)内,记录到779例中风、1233例MI和4112例死亡。在调整年龄、收缩压、体重指数、吸烟、估计肾小球滤过率、Charlson合并症指数评分、抗高血压治疗、他汀类药物、阿司匹林和病变冠状动脉数量后,ePWV与全因死亡率(每1 m/s的风险比[HR]为1.13;95%CI,1.05 - 1.21)和MI(每1 m/s的HR为1.23,95%CI,1.09 - 1.39)相关。与传统风险因素相比,包含ePWV的调整模型与死亡率辨别力的轻微但可能无临床相关性的增加相关,有ePWV时为76.63%,无ePWV时为76.56%,<0.05。
在稳定型心绞痛患者中,ePWV除传统风险因素外还与全因死亡率和MI相关。然而,死亡率的额外预测在临床上并无显著改善。