Kang Dain, Jung Jin, Park Silvia, Cho Byung-Sik, Kim Hee-Je, Kim Yeojae, Lee Jong-Mi, Kim Hoon Seok, Ahn Ari, Kim Myungshin, Kim Yonggoo
Catholic Genetic Laboratory Center, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul 06591, Korea.
Department of Biomedicine & Health Sciences, Graduate School, The Catholic University of Korea, Seoul 06591, Korea.
J Clin Med. 2022 Apr 23;11(9):2378. doi: 10.3390/jcm11092378.
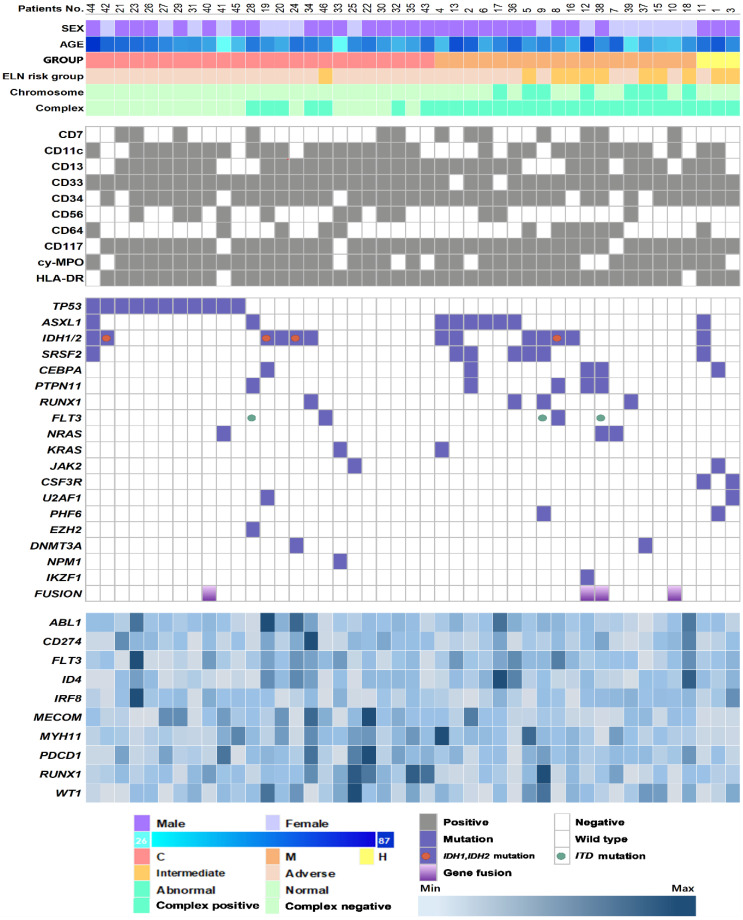
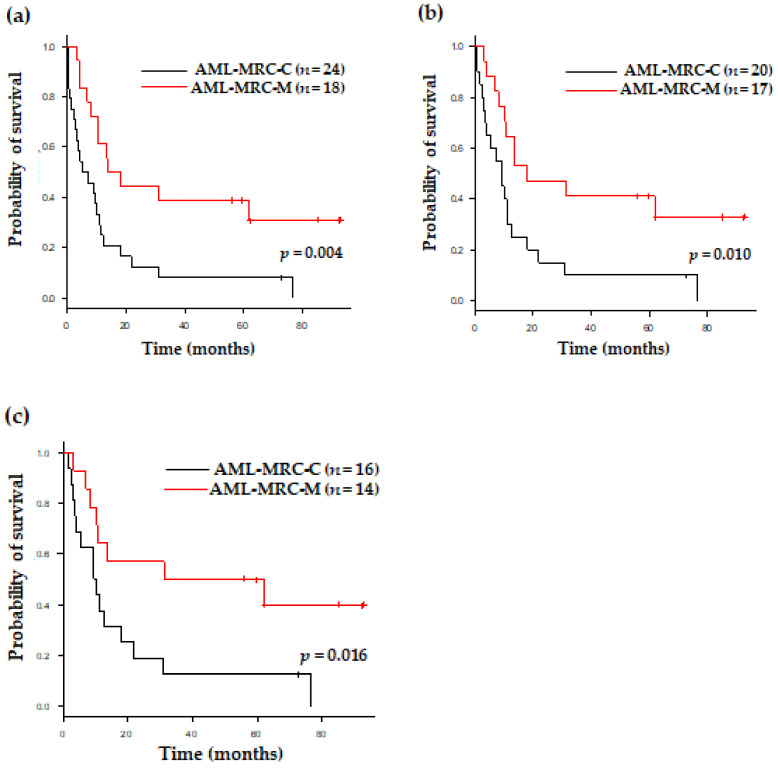
Acute myeloid leukemia with myelodysplasia-related changes (AML-MRC) includes heterogeneous conditions such as previous history and specific cytogenetic and morphological properties. In this study, we analyze genetic aberrations using an RNA-based next-generation sequencing (NGS) panel assay in 45 patients with AML-MRC and detect 4 gene fusions of KMT2A-SEPT9, KMT2A-ELL, NUP98-NSD1, and RUNX1-USP42 and 81 somatic mutations. Overall, all patients had genetic aberrations comprising of not only cytogenetic changes, but also gene fusions and mutations. We also demonstrated several characteristic genetic mutations according to the AML-MRC subgroup. TP53 was the most commonly mutated gene (n = 11, 24%) and all were found in the AML-MRC subgroup with myelodysplastic syndrome-defining cytogenetic abnormalities (AML-MRC-C) (p = 0.002). These patients showed extremely poor overall survival not only in AML-MRC, but also within the AML-MRC-C subgroup. The ASXL1 (n = 9, 20%) and SRSF2 (n = 7, 16%) mutations were associated with the AML-MRC subgroup with >50% dysplasia in at least two lineages (AML-MRC-M) and were frequently co-mutated (55%, 6/11, p < 0.001). Both mutations could be used as surrogate markers to diagnose AML-MRC, especially when the assessment of multilineage dysplasia was difficult. IDH1/IDH2 (n = 13, 29%) were most commonly mutated in AML-MRC, followed by CEBPA (n = 5, 11%), PTPN11 (n = 5, 11%), FLT3 (n = 4, 9%), IDH1 (n = 4, 9%), and RUNX1 (n = 4, 9%). These mutations were not limited in any AML-MRC subgroup and could have more significance as a risk factor or susceptibility marker for target therapy in not only AML-MRC, but also other AML categories.
伴有骨髓发育异常相关改变的急性髓系白血病(AML-MRC)包括具有不同情况的病例,如既往病史以及特定的细胞遗传学和形态学特征。在本研究中,我们使用基于RNA的二代测序(NGS) panel检测法分析了45例AML-MRC患者的基因畸变情况,检测到4种基因融合,即KMT2A-SEPT9、KMT2A-ELL、NUP98-NSD1和RUNX1-USP42,以及81种体细胞突变。总体而言,所有患者都存在基因畸变,不仅包括细胞遗传学改变,还包括基因融合和突变。我们还根据AML-MRC亚组展示了几种特征性的基因突变。TP53是最常发生突变的基因(n = 11,24%),且均见于伴有定义骨髓发育异常综合征的细胞遗传学异常的AML-MRC亚组(AML-MRC-C)(p = 0.002)。这些患者不仅在AML-MRC中,而且在AML-MRC-C亚组内总体生存率都极低。ASXL1(n = 9,20%)和SRSF2(n = 7,16%)突变与至少两个谱系中发育异常>50%的AML-MRC亚组(AML-MRC-M)相关,且经常共同突变(55%),6/11,p < 0.001)。这两种突变都可作为诊断AML-MRC的替代标志物,尤其是在难以评估多谱系发育异常时。IDH1/IDH2(n = 13,29%)在AML-MRC中最常发生突变,其次是CEBPA(n = 5,11%)、PTPN11(n = 5,11%)、FLT3(n = 4,9%)、IDH1(n = 4,9%)和RUNX1(n = 4,9%)。这些突变不限于任何AML-MRC亚组,并且作为危险因素或易感性标志物,不仅在AML-MRC中,而且在其他AML类型中对于靶向治疗可能具有更大的意义。