Division of Epidemiology, School of Public Health, University of California, Berkeley, 2121 Berkeley Way West, Berkeley, CA, 94704, USA.
Department of Health Policy and Management, Yale School of Public Health, Yale University, 60 College St, New Haven, CT, 06510, USA.
BMC Public Health. 2022 May 14;22(1):977. doi: 10.1186/s12889-022-12997-1.
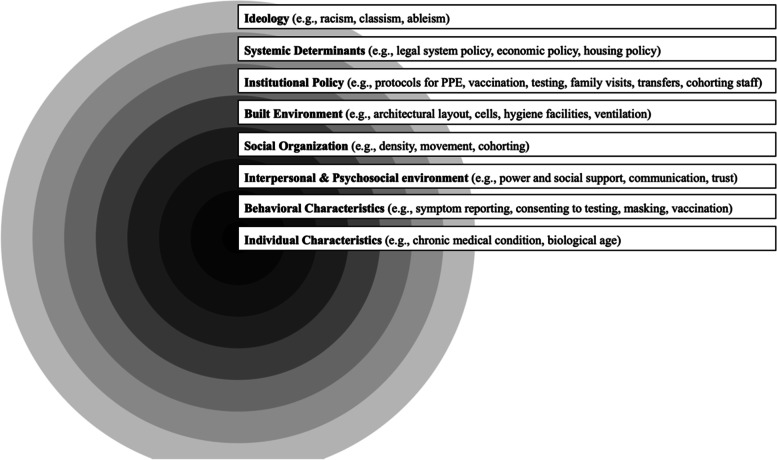
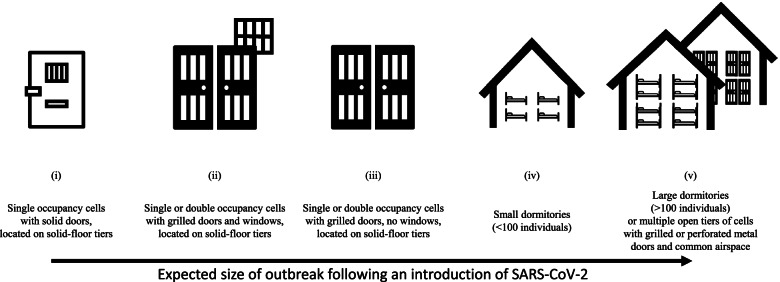
People incarcerated in US prisons have been disproportionately harmed by the COVID-19 pandemic. That prisons are such efficient superspreading environments can be attributed to several known factors: small, communal facilities where people are confined for prolonged periods of time; poor ventilation; a lack of non-punitive areas for quarantine/medical isolation; and staggeringly high numbers of people experiencing incarceration, among others. While health organizations have issued guidance on preventing and mitigating COVID-19 infection in carceral settings, little is known about if, when, and how recommendations have been implemented. We examined factors contributing to containment of one of the first California prison COVID-19 outbreaks and remaining vulnerabilities using an adapted multi-level determinants framework to systematically assess infectious disease risk in carceral settings.
Case study employing administrative data; observation; and informal discussions with: people incarcerated at the prison, staff, and county public health officials.
Outbreak mitigation efforts were characterized by pre-planning (e.g., designation of ventilated, single-occupancy quarantine) and a quickly mobilized inter-institutional response that facilitated systematic, voluntary rapid testing. However, several systemic- and institutional-level vulnerabilities were unaddressed hindering efforts and posing significant risk for future outbreaks, including insufficient decarceration, continued inter-facility transfers, incomplete staff cohorting, and incompatibility between built environment features (e.g., dense living conditions) and public health recommendations.
Our adapted framework facilitates systematically assessing prison-based infectious disease outbreaks and multi-level interventions. We find implementing some recommended public health strategies may have contributed to outbreak containment. However, even with a rapidly mobilized, inter-institutional response, failure to decarcerate created an overreliance on chance conditions. This left the facility vulnerable to future catastrophic outbreaks and may render standard public health strategies - including the introduction of effective vaccines - insufficient to prevent or contain those outbreaks.
在美国监狱中被监禁的人受到 COVID-19 大流行的不成比例的伤害。监狱是如此高效的超级传播环境,可以归因于几个已知因素:小而公共的设施,人们被长时间监禁;通风不良;缺乏非惩罚性的隔离/医学隔离区;以及被监禁人数极高,等等。虽然卫生组织已经发布了在监禁环境中预防和减轻 COVID-19 感染的指南,但对于建议是否、何时以及如何实施知之甚少。我们使用适应性多层次决定因素框架系统地评估了监禁环境中的传染病风险,以检查导致加利福尼亚州首例监狱 COVID-19 爆发得到控制和剩余脆弱性的因素。
案例研究采用行政数据;观察;以及与:监狱中的囚犯、工作人员和县公共卫生官员进行非正式讨论。
爆发缓解工作的特点是预先规划(例如,指定通风、单人隔离检疫)和快速动员机构间反应,这有助于系统、自愿的快速检测。然而,一些系统和机构层面的脆弱性未得到解决,这阻碍了努力并对未来爆发构成重大风险,包括监禁不足、持续的机构间转移、工作人员不完全分组以及建筑环境特征(例如,密集的居住条件)与公共卫生建议之间的不兼容性。
我们的适应性框架有助于系统地评估监狱内传染病爆发和多层次干预措施。我们发现,实施一些推荐的公共卫生策略可能有助于控制疫情爆发。然而,即使有快速动员的机构间反应,不进行减刑也会导致过度依赖偶然条件。这使该设施容易受到未来灾难性爆发的影响,并且可能使标准的公共卫生策略(包括引入有效的疫苗)不足以预防或控制这些爆发。