Department of Physical Therapy, University of Miami, Coral Gables, FL, USA.
Department of Neurology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, USA.
Restor Neurol Neurosci. 2022;40(2):73-84. doi: 10.3233/RNN-211227.
The sequelae of stoke, including the loss and recovery of function, are strongly linked to the mechanisms of neuroplasticity. Rehabilitation and non-invasive brain stimulation (NIBS) paradigms have shown promise in modulating corticomotor neuroplasticity to promote functional recovery in individuals post-stroke. However, an important limitation to these approaches is that while stroke recovery depends on the mechanisms of neuroplasticity, those mechanisms may themselves be altered by a stroke.
Compare Transcranial Magnetic Stimulation (TMS)-based assessments of efficacy of mechanism of neuroplasticity between individuals post-stroke and age-matched controls.
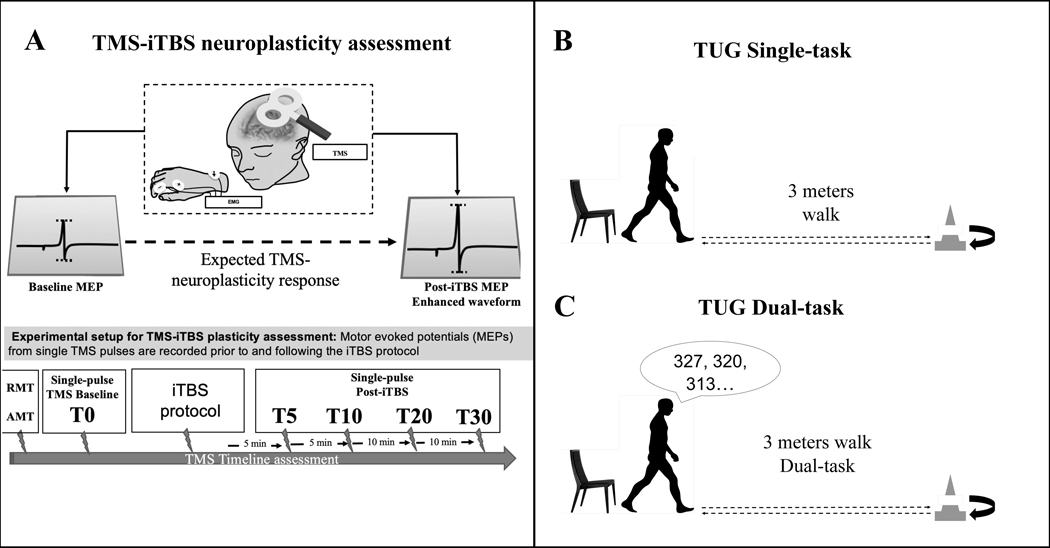
Thirty-two participants (16 post-stroke, 16 control) underwent an assessment of mechanisms of neuroplasticity, measured by the change in amplitude of motor evoked potentials elicited by single-pulse TMS 10-20 minutes following intermittent theta-burst stimulation (iTBS), and dual-task effect (DTE) reflecting cognitive-motor interference (CMI). In stroke participants, we further collected: time since stroke, stroke type, location, and Stroke Impact Scale 16 (SIS-16).
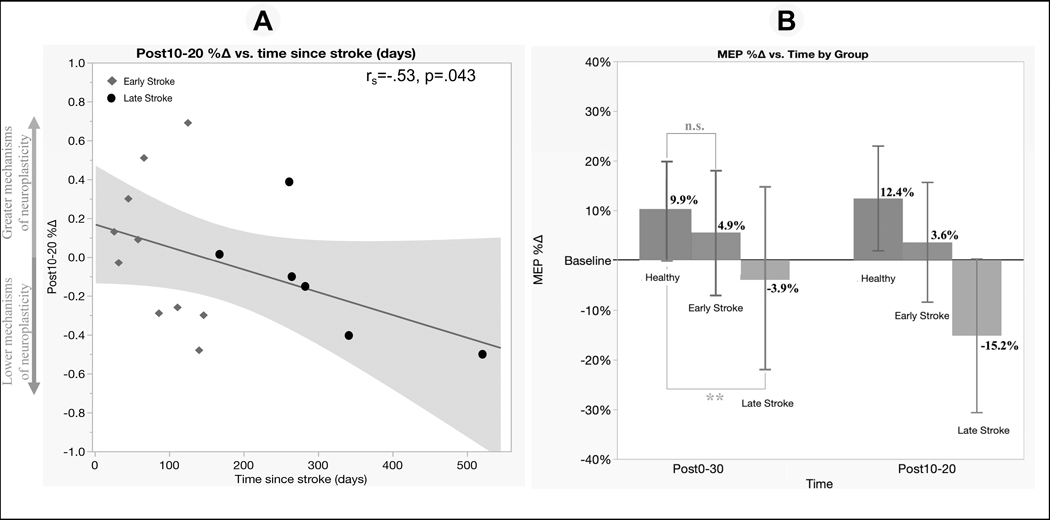
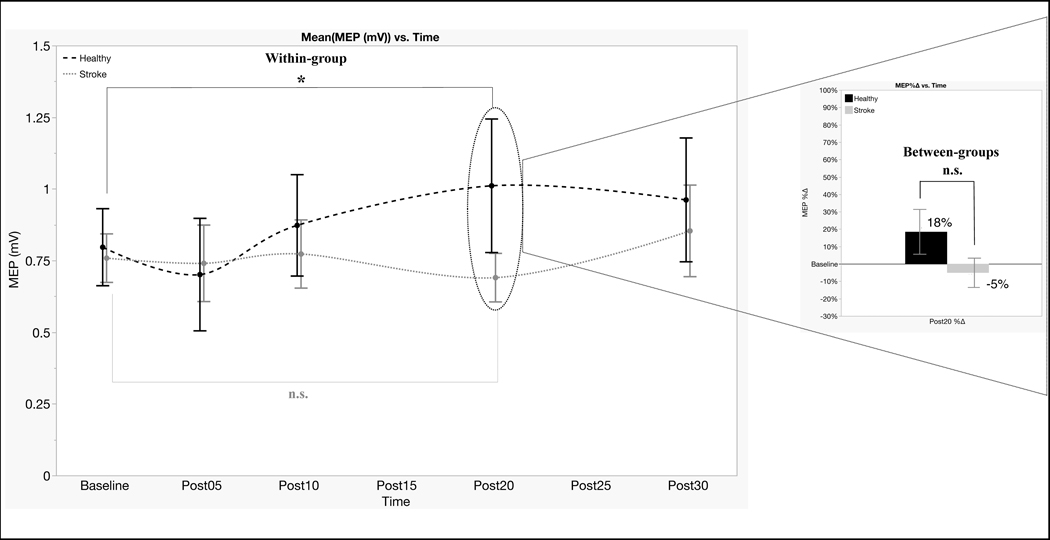
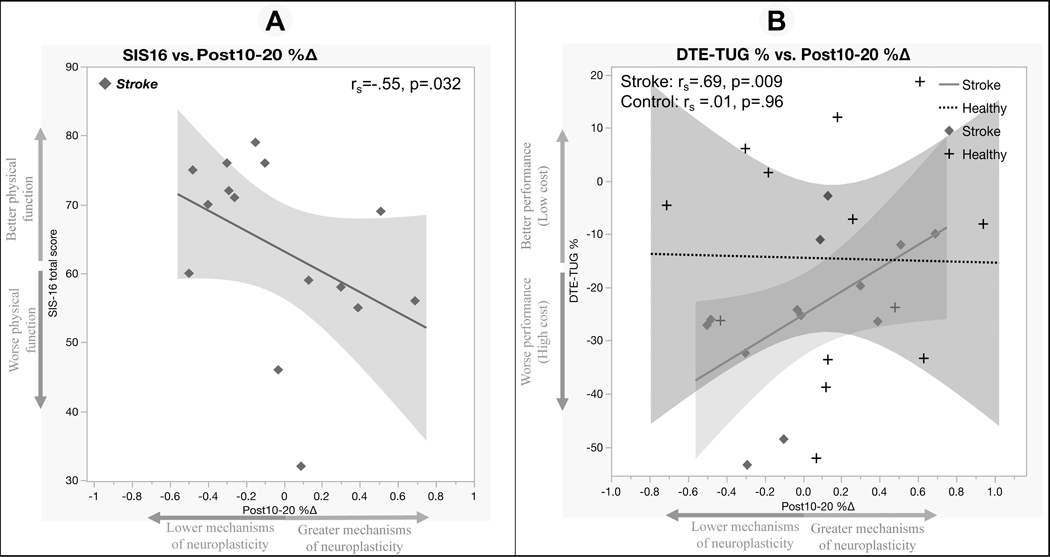
Although there was no between-group difference in the efficacy of TMS-iTBS neuroplasticity mechanism (p = 0.61, η2 = 0.01), the stroke group did not exhibit the expected facilitation to TMS-iTBS (p = 0.60, η2 = 0.04) that was shown in the control group (p = 0.016, η2 = 0.18). Sub-cohort analysis showed a trend toward a difference between those in the late-stage post-stroke and the control group (p = 0.07, η2 = 0.12). Within the post-stroke group, we found significant relationships between TMS-iTBS neuroplasticity and time since stroke onset, physical function (SIS-16), and CMI (all rs > |0.53| and p-values < 0.05).
In this proof-of-principle study, our findings suggested altered mechanisms of neuroplasticity in post-stroke patients which were dependent on time since stroke and related to motor function. TMS-iTBS neuroplasticity assessment and its relationship with clinical functional measures suggest that TMS may be a useful tool to study post-stroke recovery. Due to insufficient statistical power and high variability of the data, generalization of the findings will require replication of the results in a larger, better-characterized cohort.
中风的后遗症,包括功能的丧失和恢复,与神经可塑性机制密切相关。康复和非侵入性脑刺激(NIBS)范式已显示出在调节皮质运动神经可塑性方面的潜力,以促进中风后个体的功能恢复。然而,这些方法的一个重要局限性是,虽然中风恢复依赖于神经可塑性机制,但这些机制本身可能会被中风改变。
比较中风后个体和年龄匹配对照组之间基于经颅磁刺激(TMS)的神经可塑性机制疗效评估。
32 名参与者(16 名中风后,16 名对照组)接受了神经可塑性机制的评估,通过单脉冲 TMS 后 10-20 分钟的运动诱发电位幅度变化来测量,该变化由间歇 theta 爆发刺激(iTBS)引起,以及反映认知-运动干扰(CMI)的双重任务效应(DTE)。在中风参与者中,我们进一步收集了:中风发病时间、中风类型、位置和中风影响量表 16(SIS-16)。
尽管 TMS-iTBS 神经可塑性机制的组间疗效无差异(p=0.61,η2=0.01),但中风组并未表现出对照组中预期的 TMS-iTBS 易化作用(p=0.60,η2=0.04)。亚组分析显示,晚期中风组与对照组之间存在差异的趋势(p=0.07,η2=0.12)。在中风组中,我们发现 TMS-iTBS 神经可塑性与中风发病时间、身体功能(SIS-16)和 CMI 之间存在显著关系(所有 rs>|0.53|,p 值<0.05)。
在这项原理验证研究中,我们的发现表明中风后患者的神经可塑性机制发生改变,这取决于中风发病时间,并与运动功能相关。TMS-iTBS 神经可塑性评估及其与临床功能测量的关系表明,TMS 可能是研究中风后恢复的有用工具。由于统计能力不足和数据的高度变异性,需要在更大、特征更好的队列中复制结果来推广发现。