School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia.
Department of Statistics, Haramaya University, Haramaya, Ethiopia.
BMJ Open. 2022 May 18;12(5):e054975. doi: 10.1136/bmjopen-2021-054975.
Perinatal mortality is an important outcome indicator for newborn care and directly mirrors the quality of prenatal, intra partum and newborn care. Therefore, this study was aimed at estimating perinatal mortality and its predictors in Eastern Ethiopia using data from Kersa Health and Demographic Surveillance System (KHDSS).
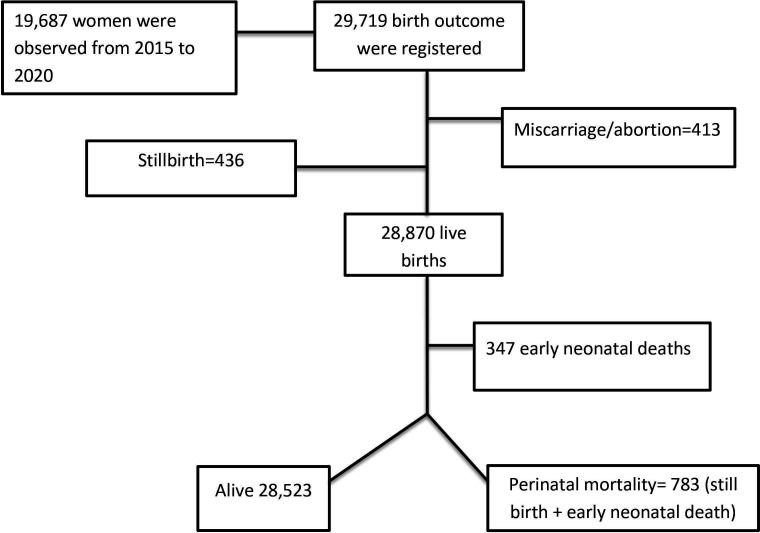
DESIGN, SETTINGS AND PARTICIPANTS: An open dynamic cohort design was employed among pregnant women from 2015 to 2020 at KHDSS. A total of 19 687 women were observed over the period of 6 years, and 29 719 birth outcomes were registered.
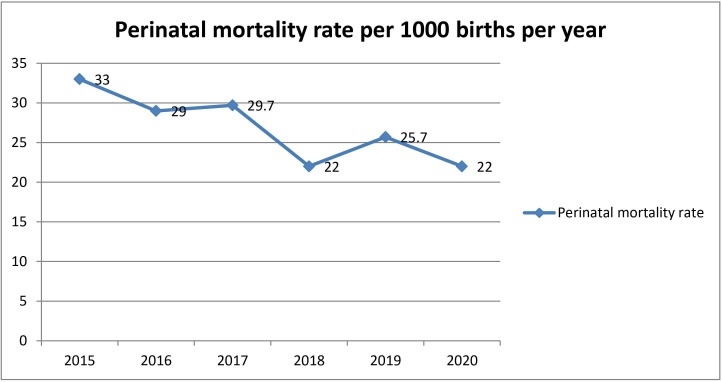
Perinatal mortality rate was estimated for each year of cohort and the cumulative of 6 years. Predictors of perinatal mortality are identified.
From a total of 29 306 births 783 (26.72 deaths per 1000 births; 95% CI 24.88 to 28.66) deaths were occurred during perinatal period. Rural residence (adjusted OR (AOR)=3.43; 95% CI 2.04 to 5.76), birth weight (low birth weight, AOR=3.98; 95% CI 3.04 to 5.20; big birth weight, AOR=2.51; 95% CI 1.76 to 3.57), not having antenatal care (ANC) (AOR=1.67; 95% CI 1.29 to 2.17) were associated with higher odds of perinatal mortality whereas the parity (multipara, AOR=0.46; 95% CI 0.34 to 0.62; grand multipara, AOR=0.31; 95% CI 0.21 to 0.47) was associated with lower odds of perinatal mortality.
The study revealed relatively high perinatal mortality rate. Place of residence, ANC, parity and birth weight were identified as predictors of perinatal mortality. Devising strategies that enhance access to and utilisations of ANC services with due emphasis for rural residents, primipara mothers and newborn with low and big birth weights may be crucial for reducing perinatal mortality.
围产儿死亡率是新生儿护理的一个重要结局指标,直接反映了产前、产时和新生儿护理的质量。因此,本研究旨在利用来自埃塞俄比亚东部克尔萨健康和人口监测系统(KHDSS)的数据,估计围产儿死亡率及其预测因素。
设计、地点和参与者:采用 2015 年至 2020 年在 KHDSS 的孕妇开放式动态队列设计。在 6 年期间共观察了 19687 名妇女,登记了 29306 例分娩结局。
估计了每年队列的围产儿死亡率和 6 年的累积死亡率。确定了围产儿死亡率的预测因素。
在总共 29306 例分娩中,有 783 例(每 1000 例活产死亡 26.72 例;95%CI 24.88 至 28.66)在围产期死亡。农村居民(校正比值比(AOR)=3.43;95%CI 2.04 至 5.76)、出生体重(低出生体重,AOR=3.98;95%CI 3.04 至 5.20;巨大儿出生体重,AOR=2.51;95%CI 1.76 至 3.57)、没有产前保健(ANC)(AOR=1.67;95%CI 1.29 至 2.17)与围产儿死亡率的几率较高相关,而产次(多产妇,AOR=0.46;95%CI 0.34 至 0.62;经产妇,AOR=0.31;95%CI 0.21 至 0.47)与围产儿死亡率的几率较低相关。
本研究显示出相对较高的围产儿死亡率。居住地、ANC、产次和出生体重被确定为围产儿死亡率的预测因素。制定策略,增加农村居民、初产妇和低出生体重及巨大儿出生体重新生儿获得和利用 ANC 服务的机会,可能是降低围产儿死亡率的关键。