Department of Cardiology, Functional and Ultrasound Diagnostics, Sechenov University, Moskva, Moskva, Russian Federation
Department of Cardiology, Functional and Ultrasound Diagnostics, Sechenov University, Moskva, Moskva, Russian Federation.
Open Heart. 2022 May;9(1). doi: 10.1136/openhrt-2021-001936.
To determine the impact of sodium-dependent glucose type 2 cotransporter inhibitors on the renal function in acute heart failure.
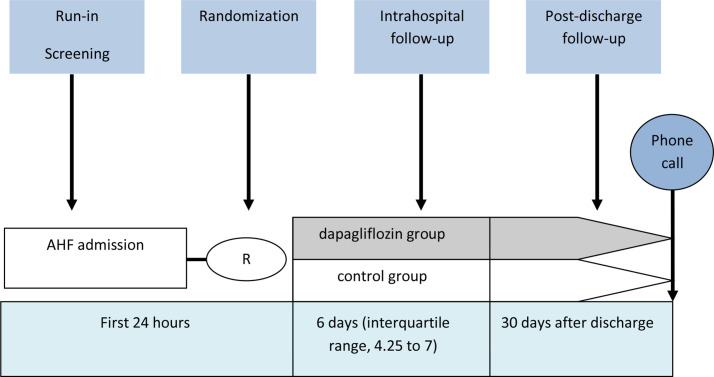
In a single-centre, controlled, randomised study, patients were prescribed dapagliflozin in addition to standard therapy, or were in receipt of standard therapy. The prespecified outcome was renal function deterioration; the secondary outcomes were the development of resistance to diuretics, weight loss, death during hospitalisation and the rehospitalisation or death for any reason within 30 days following discharge.
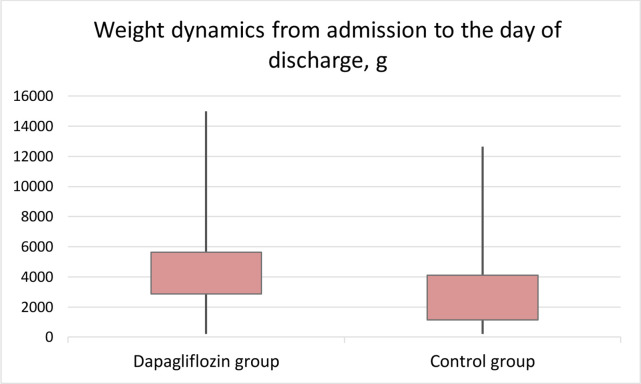
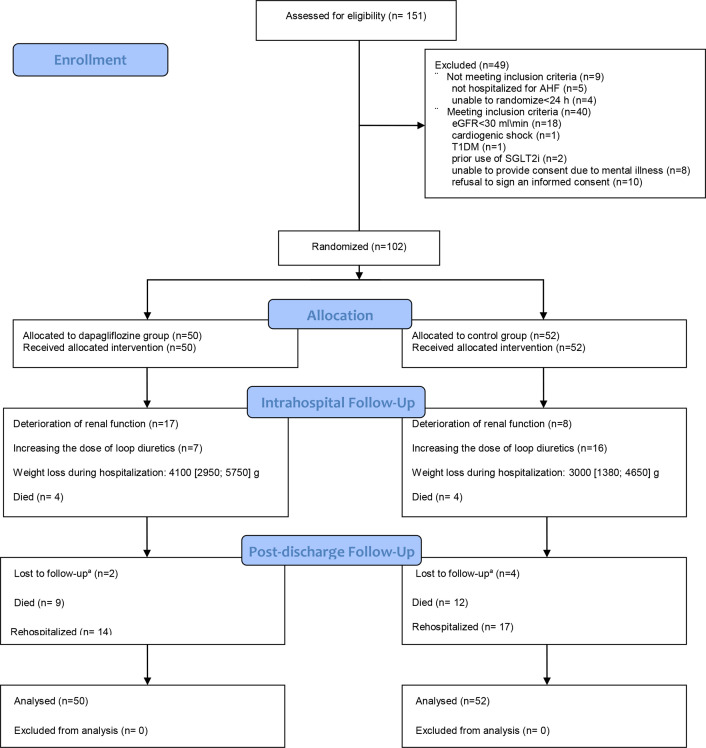
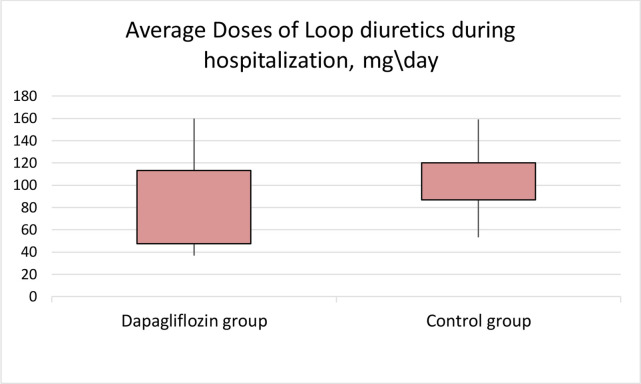
102 patients were included (73.4±11.7 years, 57.8% men). The average left ventricular ejection fraction was 44.9%±14.7%, the average N-terminal prohormone of brain natriuretic peptide (NT-proBNP) was 4706 (1757; 11 244) pg/mL, the average estimated glomerular filtration rate (eGFR) was 51.6±19.5 mL/min. eGFR decreased 48 hours after randomisation in the dapagliflozin group (-4.2 (-11.03; 2.28) mL/min vs 0.3 (-6; 6) mL/min; p=0.04) but did not differ between the groups on discharge (54.71±19.18 mL/min and 58.92±24.65 mL/min; p=0.36). The incidence of worsening renal function did not differ (34.4% vs 15.2%; p=0.07). In the dapagliflozin group, there was less tendency to increase the dose of loop diuretics (14% vs 30%; p=0.048), lower average doses of loop diuretics (78.46±38.95 mg/day vs 102.82±31.26 mg/day; p=0.001) and more significant weight loss (4100 (2950; 5750) g vs 3000 (1380; 4650) g; p=0.02). In-hospital mortality was 7.8% (4(8%) in the dapagliflozin and 4 (7.7%) in the control group (p=0.95). The number of deaths within 30 days following discharge in the dapagliflozin group and in the control group was 9 (19%) and 12 (25%), p=0.55; the number of rehospitalisations was 14 (29%) and 17 (35%), respectively (p=0.51).
The use of dapagliflozin was associated with a more pronounced weight loss and less need to increase diuretic therapy without significant deterioration of the renal function. Dapagliflozin did not improve the in-hospital and 30-day prognosis after discharge.
N04778787.
评估钠-葡萄糖共转运蛋白 2 型抑制剂对急性心力衰竭患者肾功能的影响。
在一项单中心、对照、随机研究中,给予达格列净联合标准治疗,或给予标准治疗。预设的结局是肾功能恶化;次要结局是利尿剂抵抗的发生、体重减轻、住院期间死亡以及出院后 30 天内因任何原因再次住院或死亡。
共纳入 102 例患者(73.4±11.7 岁,57.8%为男性)。平均左心室射血分数为 44.9%±14.7%,平均脑钠肽前体 N 端(NT-proBNP)为 4706(1757;11244)pg/ml,平均估算肾小球滤过率(eGFR)为 51.6±19.5ml/min。达格列净组在随机分组后 48 小时 eGFR 下降(-4.2(-11.03;2.28)ml/min 与 0.3(-6;6)ml/min;p=0.04),但出院时两组间无差异(54.71±19.18ml/min 和 58.92±24.65ml/min;p=0.36)。肾功能恶化的发生率无差异(34.4%与 15.2%;p=0.07)。在达格列净组中,利尿剂剂量增加的趋势较小(14%与 30%;p=0.048),平均利尿剂剂量较低(78.46±38.95mg/天与 102.82±31.26mg/天;p=0.001),体重减轻更显著(4100(2950;5750)g 与 3000(1380;4650)g;p=0.02)。院内死亡率为 7.8%(4(8%)在达格列净组和 4(7.7%)在对照组(p=0.95)。达格列净组和对照组出院后 30 天内死亡的人数分别为 9(19%)和 12(25%)(p=0.55),再住院的人数分别为 14(29%)和 17(35%)(p=0.51)。
达格列净的使用与更明显的体重减轻和减少利尿剂治疗的需求相关,而肾功能无显著恶化。达格列净并未改善住院和出院后 30 天的预后。
N04778787。