Department of Public Health and Community Medicine, Faculty of Medicine, Beni-Suef University, Beni-Suef, 62521, Egypt.
Department of Emergency Medicine, University of Maryland School of Medicine, Baltimore, MD, 21201, USA.
BMC Emerg Med. 2022 May 28;22(1):90. doi: 10.1186/s12873-022-00653-1.
Numerous trauma scoring systems have been developed in an attempt to accurately and efficiently predict the prognosis of emergent trauma cases. However, it has been questioned as to whether the accuracy and pragmatism of such systems still hold in lower-resource settings that exist in many hospitals in lower- and middle-income countries (LMICs). In this study, it was hypothesized that the physiologically-based Revised Trauma Score (RTS), Mechanism/Glasgow Coma Scale/Age/Pressure (MGAP) score, and Glasgow Coma Scale/Age/Pressure (GAP) score would be effective at predicting mortality outcomes using clinical data at presentation in a representative LMIC hospital in Upper Egypt.
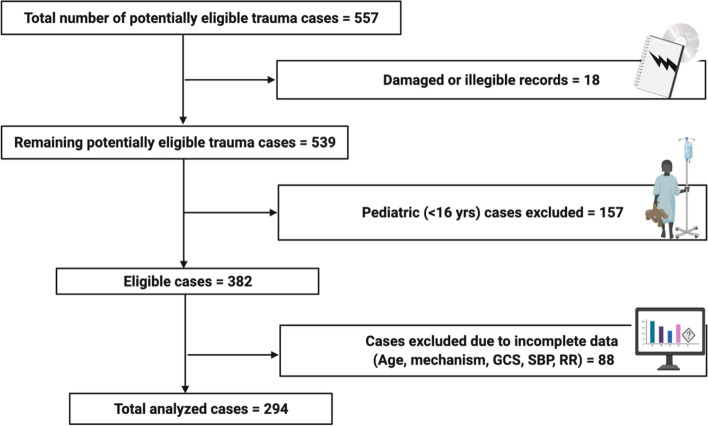
This was a retrospective analysis of the medical records of trauma patients at Beni-Suef University Hospital. Medical records of all trauma patients admitted to the hospital over the 8-month period from January to August 2016 were reviewed. For each case, the RTS, MGAP, and GAP scores were calculated using clinical data at presentation, and mortality prediction was correlated to the actual in-hospital outcome.
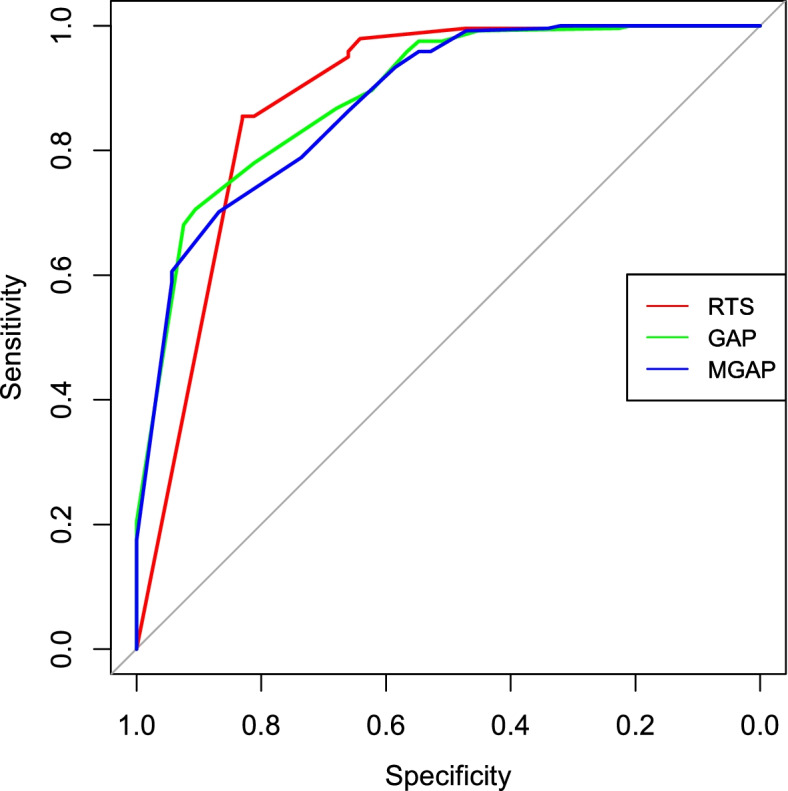
The Area Under the Receiver Operating Characteristic (AUROC) was calculated to be 0.879, 0.890, and 0.881 for the MGAP, GAP, and RTS respectively, with all three scores showing good discriminatory ability. With regards to prevalence-dependent statistics, all three scores demonstrated efficacy in ruling out mortality upon presentation with negative predictive values > 95%, while the MGAP score best captured the mortality subgroup with a sensitivity of 94%. Adjustment of cutoff scores showed a steep trade-off between optimizing the positive predictive values versus the sensitivities.
The RTS, MGAP, and GAP all showed good discriminatory capabilities per AUROC. Given the relative simplicity and potentially added clinical benefit in capturing critically ill patients, the MGAP score should be further studied for stratifying risk of incoming trauma patients to the emergency department, allowing for more efficacious triage of patients in lower-resource healthcare settings.
为了准确、有效地预测急诊创伤病例的预后,已经开发了许多创伤评分系统。然而,人们质疑这些系统的准确性和实用性是否仍然适用于中低收入国家(LMIC)许多医院中存在的资源较少的环境。在这项研究中,假设生理修订创伤评分(RTS)、机制/格拉斯哥昏迷评分/年龄/压力(MGAP)评分和格拉斯哥昏迷评分/年龄/压力(GAP)评分在使用埃及上埃及代表性 LMIC 医院就诊时的临床数据,能够有效地预测死亡率结局。
这是对 Beni-Suef 大学医院创伤患者病历的回顾性分析。回顾了 2016 年 1 月至 8 月 8 个月期间入住该医院的所有创伤患者的病历。对于每个病例,使用就诊时的临床数据计算 RTS、MGAP 和 GAP 评分,并将死亡率预测与实际住院结局相关联。
MGAP、GAP 和 RTS 的受试者工作特征曲线下面积(AUROC)分别为 0.879、0.890 和 0.881,均具有良好的区分能力。关于患病率依赖性统计,所有三个评分在呈现时排除死亡率的阴性预测值均>95%,具有疗效,而 MGAP 评分则以 94%的灵敏度最佳捕捉死亡率亚组。调整截止值显示,在优化阳性预测值与灵敏度之间存在陡峭的权衡。
RTS、MGAP 和 GAP 均根据 AUROC 显示出良好的区分能力。鉴于在捕捉危重病患者方面的相对简单性和潜在的临床获益,MGAP 评分应进一步研究,以分层进入急诊科的创伤患者的风险,从而在资源较少的医疗环境中更有效地对患者进行分诊。