Division of Infection, Immunity and Respiratory Medicine, University of Manchester, Manchester, UK.
Manchester Thoracic Oncology Centre, Manchester University NHS Foundation Trust, Manchester, UK.
Eur Respir J. 2022 Nov 24;60(5). doi: 10.1183/13993003.00483-2022. Print 2022 Nov.
Screening with low-dose computed tomography (LDCT) reduces lung cancer mortality; however, the most effective strategy for optimising participation is unknown. Here we present data from the Yorkshire Lung Screening Trial, including response to invitation, screening eligibility and uptake of community-based LDCT screening.
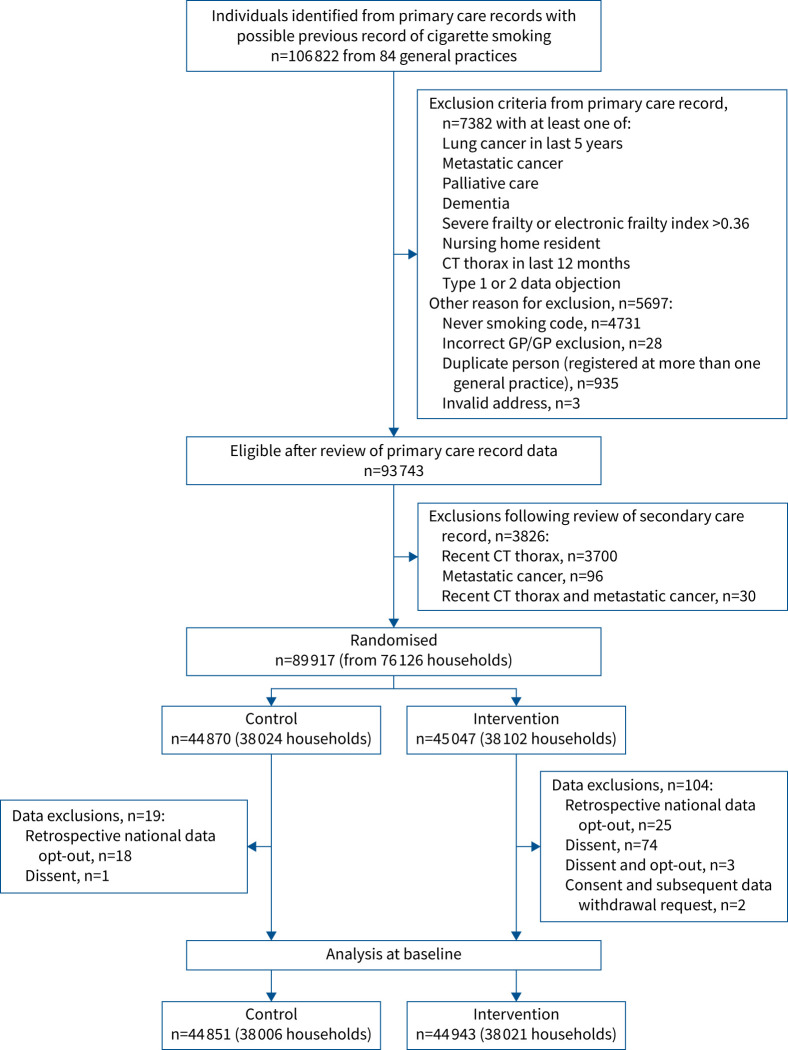
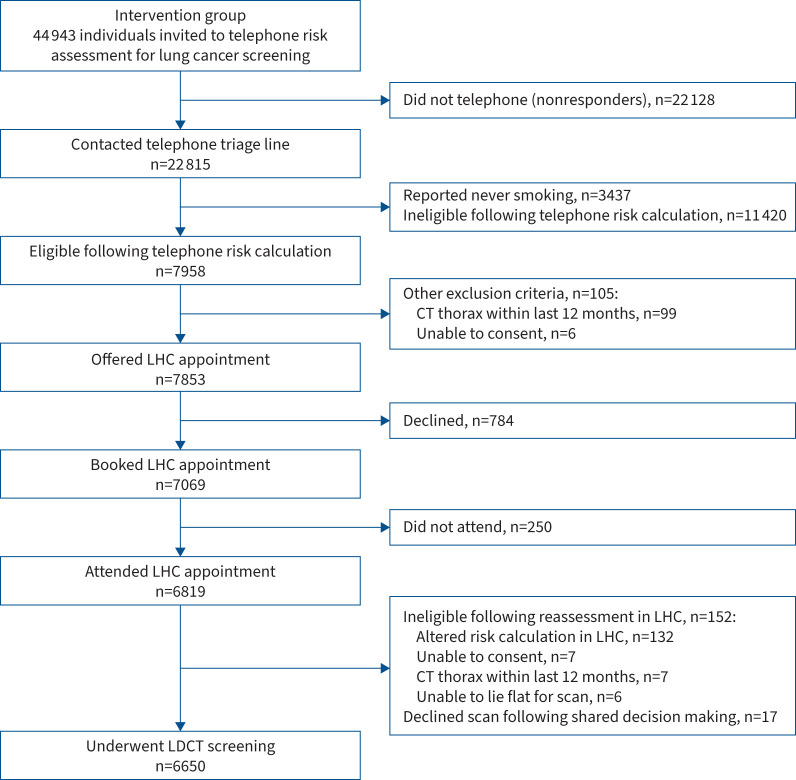
Individuals aged 55-80 years, identified from primary care records as having ever smoked, were randomised prior to consent to invitation to telephone lung cancer risk assessment or usual care. The invitation strategy included general practitioner endorsement, pre-invitation and two reminder invitations. After telephone triage, those at higher risk were invited to a Lung Health Check (LHC) with immediate access to a mobile CT scanner.
Of 44 943 individuals invited, 50.8% (n=22 815) responded and underwent telephone-based risk assessment (16.7% and 7.3% following first and second reminders, respectively). A lower response rate was associated with current smoking status (adjusted OR 0.44, 95% CI 0.42-0.46) and socioeconomic deprivation (adjusted OR 0.58, 95% CI 0.54-0.62 for the most the least deprived quintile). Of those responding, 34.4% (n=7853) were potentially eligible for screening and offered a LHC, of whom 86.8% (n=6819) attended. Lower uptake was associated with current smoking status (adjusted OR 0.73, 95% CI 0.62-0.87) and socioeconomic deprivation (adjusted OR 0.78, 95% CI 0.62-0.98). In total, 6650 individuals had a baseline LDCT scan, representing 99.7% of eligible LHC attendees.
Telephone risk assessment followed by a community-based LHC is an effective strategy for lung cancer screening implementation. However, lower participation associated with current smoking status and socioeconomic deprivation underlines the importance of research to ensure equitable access to screening.
低剂量计算机断层扫描(LDCT)筛查可降低肺癌死亡率;然而,优化参与度的最有效策略尚不清楚。在此,我们展示了来自约克郡肺癌筛查试验的数据,包括对邀请的反应、筛查资格和社区为基础的 LDCT 筛查的接受率。
从初级保健记录中确定的年龄在 55-80 岁之间、有过吸烟史的个体,在同意前进行随机分组,接受邀请进行电话肺癌风险评估或常规护理。邀请策略包括全科医生的认可、预先邀请和两次提醒邀请。经过电话分诊,那些风险较高的人被邀请参加肺部健康检查(LHC),并可立即使用移动 CT 扫描仪。
在 44943 名受邀者中,有 50.8%(n=22815)做出回应并接受了基于电话的风险评估(第一次和第二次提醒后的分别为 16.7%和 7.3%)。较低的回应率与当前吸烟状况相关(调整后的 OR 0.44,95%CI 0.42-0.46)和社会经济贫困程度相关(与最不贫困的五分位相比,调整后的 OR 0.58,95%CI 0.54-0.62)。在做出回应的人群中,有 34.4%(n=7853)有潜在的筛查资格并被提供 LHC,其中 86.8%(n=6819)参加了。较低的接受率与当前吸烟状况相关(调整后的 OR 0.73,95%CI 0.62-0.87)和社会经济贫困程度相关(调整后的 OR 0.78,95%CI 0.62-0.98)。共有 6650 人进行了基线 LDCT 扫描,占有资格参加 LHC 的人数的 99.7%。
电话风险评估后进行社区为基础的 LHC 是肺癌筛查实施的有效策略。然而,与当前吸烟状况和社会经济贫困程度相关的参与率较低,这突显了确保公平获得筛查的研究的重要性。