Department of Diabetes and Endocrinology, The Royal Melbourne Hospital, Parkville, Victoria, Australia
Department of Medicine, The University of Melbourne, Melbourne, Victoria, Australia.
BMJ Open Diabetes Res Care. 2022 Jul;10(4). doi: 10.1136/bmjdrc-2022-002880.
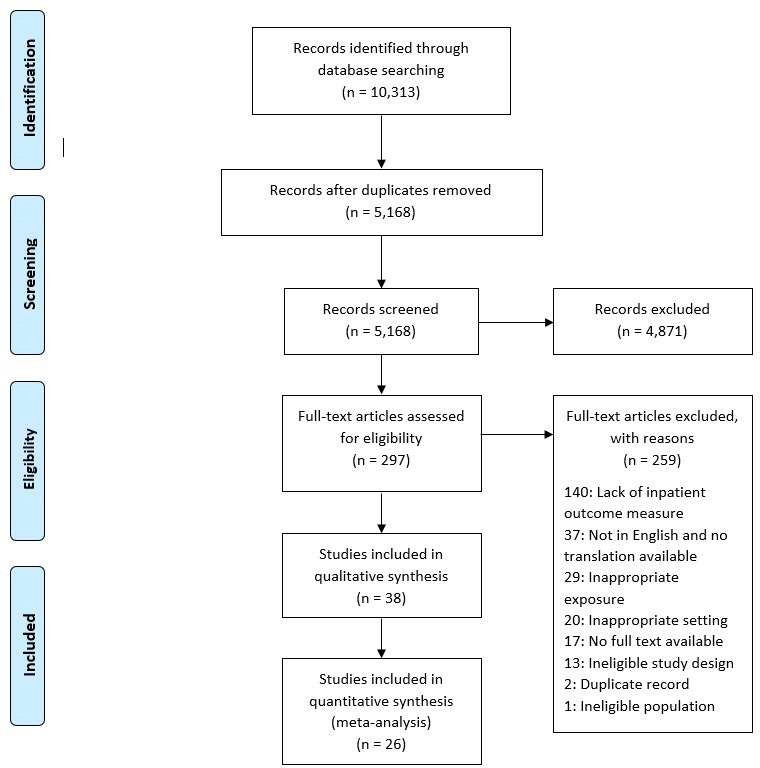
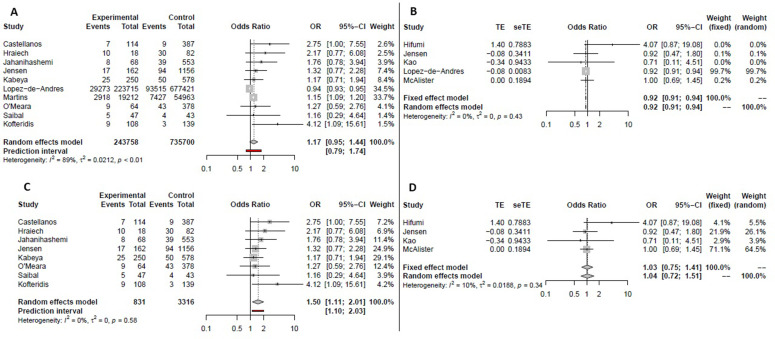
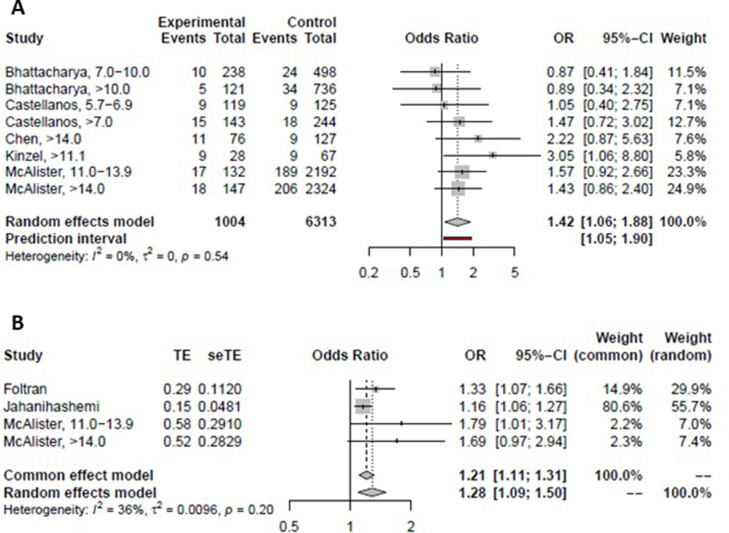
The objective of this review was to quantify the association between diabetes, hyperglycemia, and outcomes in patients hospitalized for community-acquired pneumonia (CAP) prior to the COVID-19 pandemic by conducting a systematic review and meta-analysis. Two investigators independently screened records identified in the PubMed (MEDLINE), EMBASE, CINAHL, and Web of Science databases. Cohort and case-control studies quantitatively evaluating associations between diabetes and in-hospital hyperglycemia with outcomes in adults admitted to hospital with CAP were included. Quality was assessed using the Newcastle-Ottawa Quality Assessment Scale, effect size using random-effects models, and heterogeneity using I statistics. Thirty-eight studies met the inclusion criteria. Hyperglycemia was associated with in-hospital mortality (adjusted OR 1.28, 95% CI 1.09 to 1.50) and intensive care unit (ICU) admission (crude OR 1.82, 95% CI 1.17 to 2.84). There was no association between diabetes status and in-hospital mortality (adjusted OR 1.04, 95% CI 0.72 to 1.51), 30-day mortality (adjusted OR 1.13, 95% CI 0.77 to 1.67), or ICU admission (crude OR 1.91, 95% CI 0.74 to 4.95). Diabetes was associated with increased mortality in all studies reporting >90-day postdischarge mortality and with longer length of stay only for studies reporting crude (OR 1.50, 95% CI 1.11 to 2.01) results. In adults hospitalized with CAP, in-hospital hyperglycemia but not diabetes alone is associated with increased in-hospital mortality and ICU admission. Diabetes status is associated with increased >90-day postdischarge mortality. Implications for management are that in-hospital hyperglycemia carries a greater risk for in-hospital morbidity and mortality than diabetes alone in patients admitted with non-COVID-19 CAP. Evaluation of strategies enabling timely and effective management of in-hospital hyperglycemia in CAP is warranted.
本综述的目的是通过系统评价和荟萃分析,量化糖尿病、高血糖与 COVID-19 大流行前社区获得性肺炎(CAP)住院患者结局之间的关系。两位研究者独立筛选了在 PubMed(MEDLINE)、EMBASE、CINAHL 和 Web of Science 数据库中识别出的记录。纳入了定量评估糖尿病和住院高血糖与成人因 CAP 住院患者住院期间结局之间关系的队列研究和病例对照研究。使用纽卡斯尔-渥太华质量评估量表评估质量,使用随机效应模型评估效应大小,使用 I 统计量评估异质性。38 项研究符合纳入标准。高血糖与住院死亡率(校正比值比 1.28,95%置信区间 1.09 至 1.50)和重症监护病房(ICU)入住(未校正比值比 1.82,95%置信区间 1.17 至 2.84)相关。糖尿病与住院死亡率(校正比值比 1.04,95%置信区间 0.72 至 1.51)、30 天死亡率(校正比值比 1.13,95%置信区间 0.77 至 1.67)或 ICU 入住(未校正比值比 1.91,95%置信区间 0.74 至 4.95)无关。在所有报告出院后 >90 天死亡率的研究中,糖尿病与死亡率增加相关,而在仅报告未校正(OR 1.50,95%CI 1.11 至 2.01)结果的研究中,糖尿病与住院时间延长相关。在因 CAP 住院的成年人中,住院期间高血糖而不是单纯的糖尿病与住院期间死亡率和 ICU 入住增加相关。糖尿病状态与 >90 天出院后死亡率增加相关。这对管理的启示是,与单纯糖尿病相比,住院期间高血糖与 COVID-19 非 CAP 住院患者住院期间发病率和死亡率增加的相关性更大。需要评估能够及时有效地管理 CAP 患者住院期间高血糖的策略。