Mazidi Mohsen, Mikhailidis Dimitri P, Dehghan Abbas, Jóźwiak Jacek, Covic Adrian, Sattar Naveed, Banach Maciej
Department of Twin Research and Genetic Epidemiology, King's College London, St Thomas' Hospital, Strand, London, UK.
Department of Clinical Biochemistry, Royal Free Campus, University College London Medical School, University College London (UCL), London, UK.
Arch Med Sci. 2021 Dec 14;18(4):900-911. doi: 10.5114/aoms/144905. eCollection 2022.
The reported relationship between coffee intake and renal function is poorly understood. By applying two-sample Mendelian randomization (MR) and systematic review and meta-analysis we investigated the association of caffeine and coffee intake with prevalent CKD and markers of renal function.
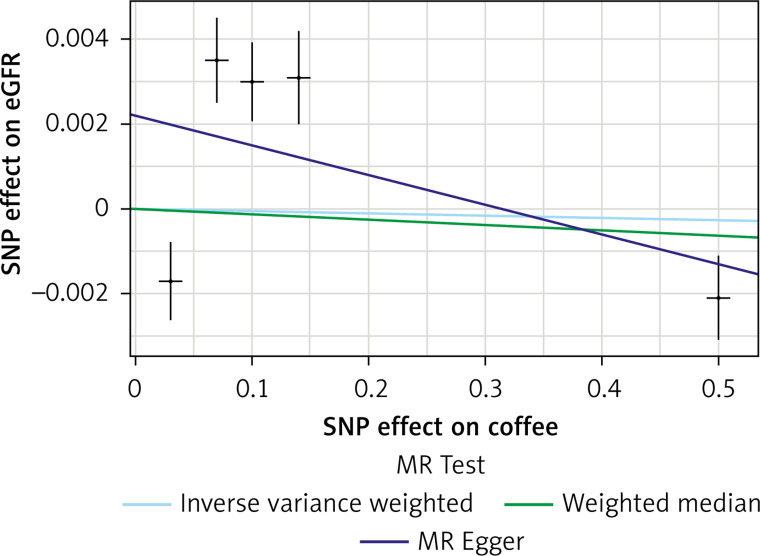
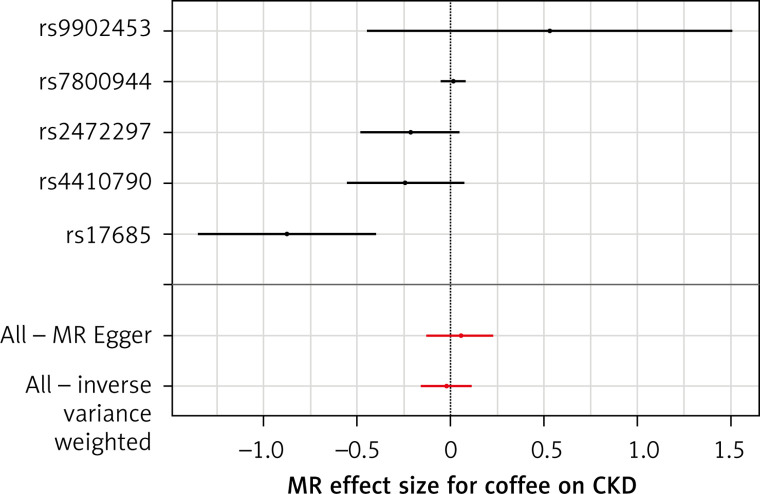
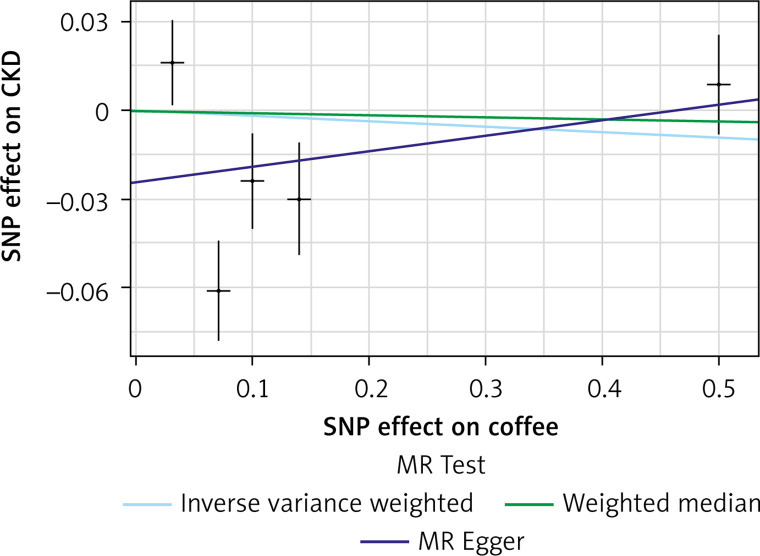
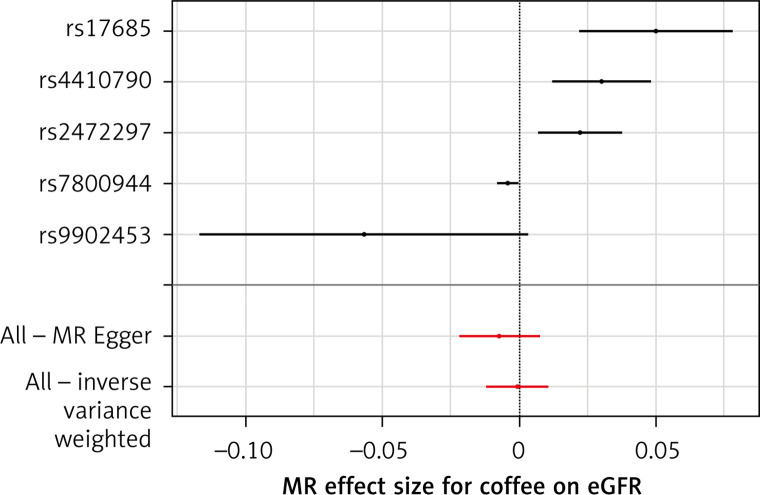
For the individual data analysis we analyzed the National Health and Nutrition Examination Surveys (NHANES) data on renal function markers and caffeine intake. MR was implemented by using summary-level data from the largest ever genome-wide association studies (GWAS) conducted on coffee intake ( = 91,462) and kidney function ( = 133,413). The inverse variance weighted method (IVW), weighted median-based method, MR-Egger, MR-RAPS, and MR-PRESSO were applied. Random effects models and generic inverse variance methods were used to synthesize quantitative and pooled data for the meta-analysis, followed by a leave-one-out method for sensitivity analysis.
Finally, we included the data of 18,436 participants; 6.9% had prevalent CKD (based on eGFR). Caffeine intake for the general population was 131.1 ±1.1 mg. The percentage of participants with CKD, by caffeine quartile, was 16.6% in the first (lowest) quartile, 13.9% in the second, 12.2% in the third and 11.0% in the top quartile ( < 0.001). After adjustment, for increasing quartiles for caffeine consumption, mean urine albumin, albumin-creatinine ratio and estimated glomerular filtration rate (GFR) did not change significantly ( > 0.234). In fully adjusted logistic regression models, there was no significant difference in chances of CKD prevalence (-trend = 0.745). In the same line, the results of MR showed no impact of coffee intake on CKD (IVW: β = -0.0191, SE = 0.069, = 0.781) or on eGFR (overall = IVW: β = -0.0005, SE = 0.005, = 0.926) either in diabetic (IVW: β = -0.006, SE = 0.009, = 0.478) or non-diabetic patients (IVW: β = -6.772, SE = 0.006, = 0.991). Results from the meta-analysis indicated that coffee consumption was not significantly associated with CKD (OR = 0.85, 95% CI: 0.71-1.02, = 0.090, = 6 studies, = 0.32). These findings were robust in sensitivity analyses.
Implementing different strategies, we detected no significant association between coffee consumption and renal function or risk of CKD.
咖啡摄入量与肾功能之间的关系目前尚不清楚。通过应用两样本孟德尔随机化(MR)以及系统评价和荟萃分析,我们研究了咖啡因和咖啡摄入量与慢性肾脏病(CKD)患病率及肾功能标志物之间的关联。
对于个体数据分析,我们分析了美国国家健康与营养检查调查(NHANES)中关于肾功能标志物和咖啡因摄入量的数据。MR分析使用了有史以来最大规模的关于咖啡摄入量(n = 91,462)和肾功能(n = 133,413)的全基因组关联研究(GWAS)的汇总数据。应用了逆方差加权法(IVW)、基于加权中位数的方法、MR-Egger、MR-RAPS和MR-PRESSO。采用随机效应模型和通用逆方差方法对荟萃分析的定量和汇总数据进行综合,随后采用留一法进行敏感性分析。
最终,我们纳入了18,436名参与者的数据;6.9%患有CKD(基于估算肾小球滤过率)。普通人群的咖啡因摄入量为131.1±1.1毫克。按咖啡因四分位数分组,CKD患者的百分比在第一(最低)四分位数中为16.6%,第二四分位数中为13.9%,第三四分位数中为12.2%,最高四分位数中为11.0%(P < 0.001)。调整后,随着咖啡因摄入量四分位数的增加,平均尿白蛋白、白蛋白-肌酐比值和估算肾小球滤过率(GFR)无显著变化(P > 0.234)。在完全调整的逻辑回归模型中,CKD患病率的几率无显著差异(P趋势 = 0.745)。同样,MR结果显示咖啡摄入量对CKD(IVW:β = -0.0191,SE = 0.069,P = 0.781)或eGFR(总体IVW:β = -0.0005,SE = 0.005,P = 0.926)均无影响,无论是在糖尿病患者(IVW:β = -0.006,SE = 0.009,P = 0.478)还是非糖尿病患者中(IVW:β = -6.772,SE = 0.006,P = 0.991)。荟萃分析结果表明,咖啡消费与CKD无显著关联(OR = 0.85,95%CI:0.71 - 1.02,P = 0.090,I² = 6项研究,P = 0.32)。这些发现在敏感性分析中是稳健的。
通过实施不同策略,我们未发现咖啡消费与肾功能或CKD风险之间存在显著关联。