Centre for Disease Modelling (CDM), York University, 4700 Keele Street, Toronto, ON, M3J1P3, Canada.
Department of Mathematics and Statistics, York University, 4700 Keele Street, Toronto, ON, M3J1P3, Canada.
BMC Public Health. 2022 Jul 15;22(1):1349. doi: 10.1186/s12889-022-13597-9.
Since December 2020, public health agencies have implemented a variety of vaccination strategies to curb the spread of SARS-CoV-2, along with pre-existing Nonpharmaceutical Interventions (NPIs). Initial strategies focused on vaccinating the elderly to prevent hospitalizations and deaths, but with vaccines becoming available to the broader population, it became important to determine the optimal strategy to enable the safe lifting of NPIs while avoiding virus resurgence.
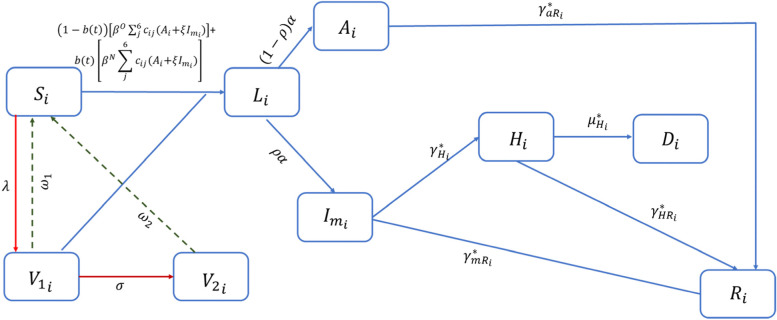
We extended the classic deterministic SIR compartmental disease-transmission model to simulate the lifting of NPIs under different vaccine rollout scenarios. Using case and vaccination data from Toronto, Canada between December 28, 2020, and May 19, 2021, we estimated transmission throughout past stages of NPI escalation/relaxation to compare the impact of lifting NPIs on different dates on cases, hospitalizations, and deaths, given varying degrees of vaccine coverages by 20-year age groups, accounting for waning immunity.
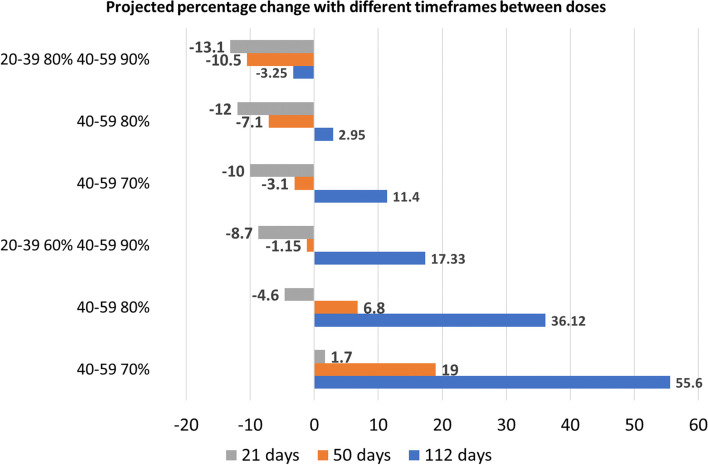
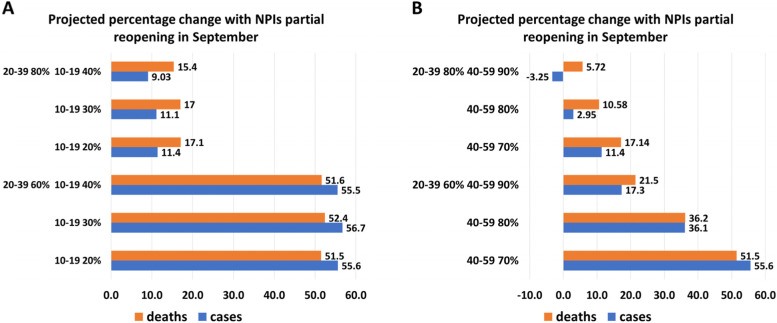
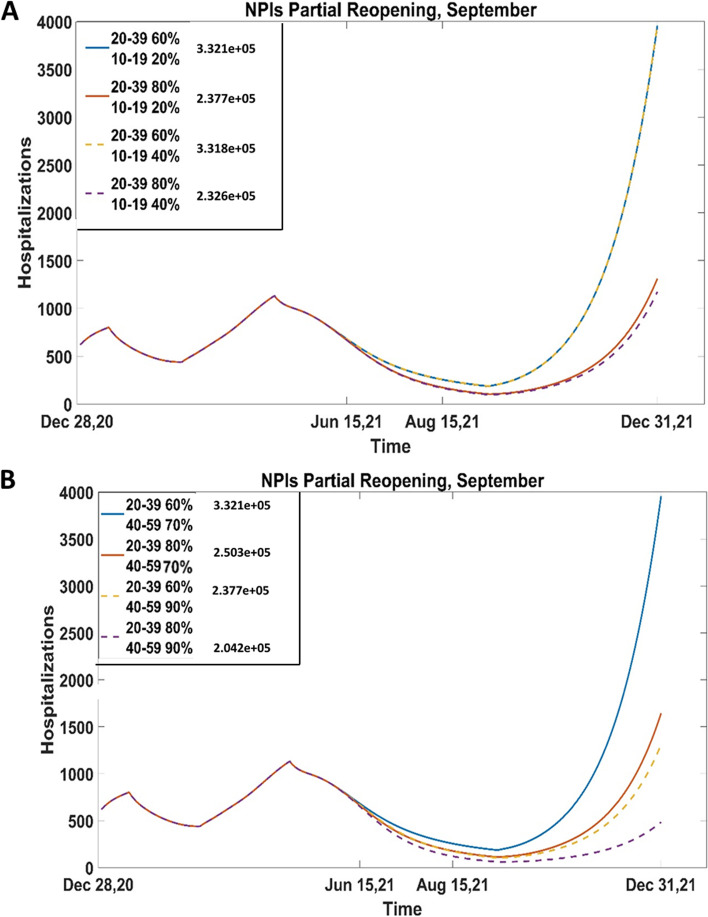
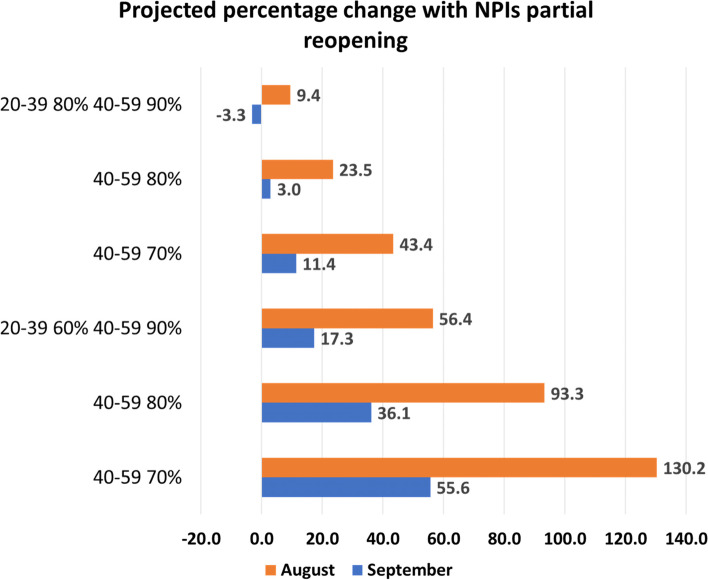
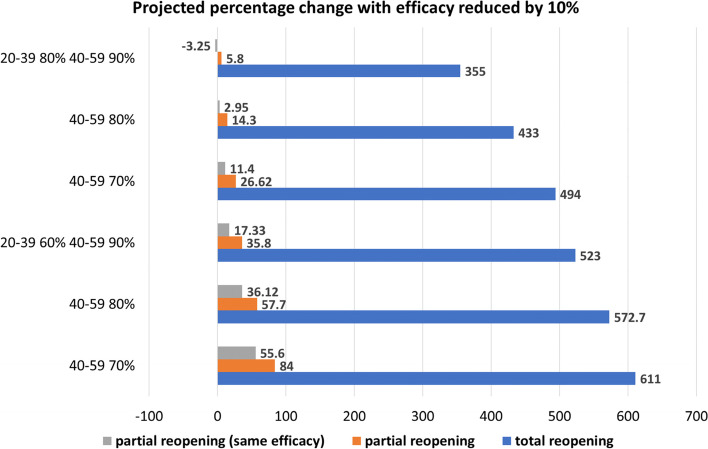
We found that, once coverage among the elderly is high enough (80% with at least one dose), the main age groups to target are 20-39 and 40-59 years, wherein first-dose coverage of at least 70% by mid-June 2021 is needed to minimize the possibility of resurgence if NPIs are to be lifted in the summer. While a resurgence was observed for every scenario of NPI lifting, we also found that under an optimistic vaccination coverage (70% coverage by mid-June, along with postponing reopening from August 2021 to September 2021) can reduce case counts and severe outcomes by roughly 57% by December 31, 2021.
Our results suggest that focusing the vaccination strategy on the working-age population can curb the spread of SARS-CoV-2. However, even with high vaccination coverage in adults, increasing contacts and easing protective personal behaviours is not advisable since a resurgence is expected to occur, especially with an earlier reopening.
自 2020 年 12 月以来,公共卫生机构实施了多种疫苗接种策略,以遏制 SARS-CoV-2 的传播,同时还采取了先前存在的非药物干预措施(NPIs)。最初的策略侧重于为老年人接种疫苗,以防止住院和死亡,但随着疫苗可供更广泛的人群使用,确定在避免病毒再次出现的情况下安全解除 NPI 的最佳策略变得很重要。
我们扩展了经典的确定性 SIR 传染病传播模型,以模拟在不同疫苗推出场景下解除 NPI 的情况。我们使用 2020 年 12 月 28 日至 2021 年 5 月 19 日期间加拿大多伦多的病例和疫苗接种数据,估计了过去 NPI 升级/放松阶段的传播情况,以比较在不同日期解除 NPI 对病例、住院和死亡的影响,考虑到不同年龄段疫苗接种覆盖率的变化,并考虑了免疫力的下降。
我们发现,一旦老年人的覆盖率足够高(至少一剂的覆盖率为 80%),主要目标年龄段是 20-39 岁和 40-59 岁,其中需要在 2021 年 6 月中旬之前实现至少 70%的第一剂覆盖率,以降低如果在夏季解除 NPI 可能出现的再次爆发的可能性。虽然在解除 NPI 的每种情况下都观察到了再次爆发,但我们还发现,在乐观的疫苗接种覆盖率(2021 年 6 月中旬覆盖率为 70%,并将重新开放从 2021 年 8 月推迟到 9 月)下,可以将 2021 年 12 月 31 日之前的病例数和严重后果减少约 57%。
我们的结果表明,将疫苗接种策略集中在工作年龄人群上可以遏制 SARS-CoV-2 的传播。然而,即使成年人的疫苗接种覆盖率很高,增加接触和放宽个人保护行为也是不可取的,因为预计会出现再次爆发,特别是在提前重新开放的情况下。